

Introduction: Preclincal murine models of primary and secondary hemophagocytic lymphohistiocytosis (HLH) have demonstrated the role of JAK/STAT signaling in propagating the cytokine-mediated hyperinflammatory state. Das et al. (Blood 2016) demonstrated that ruxolitinib (rux) effectively attenuates murine HLH, and Albeituni et al. (Blood 2019) found it superior to IFN-γ inhibition (the target of emapalumab-lzsg). A few single case reports exist in which rux was used for salvage therapy, however they report only limited clinical success and/or were used as a bridge to allogeneic stem cell transplantation. Here we present a series of three consecutive cases in which rux was employed as either salvage therapy for relapsed/refractory secondary HLH or front-line for moderate HLH manifestations. Importantly, each patient was maintained on a taper of rux which prevented recurrence and obviated the need for allogeneic transplantation. Two of the three patients have been tapered completely off rux without recurrence of either laboratory or clinical manifestations of HLH at the time of this submission.
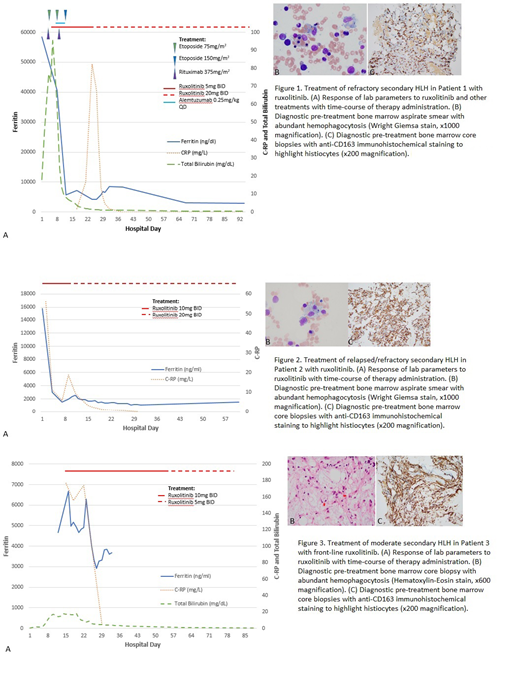
Case 1: Patient 1 is a 24 yo woman who had initially presented to an outside hospital with jaundice and was found to have a warm AIHA. She was initially started on steroids, but developed worsening anemia, fever, splenomegaly, and encephalopathy. On transfer to us she had ferritin of 58,505 ng/ml. Her bone marrow biopsy demonstrated abundant hemophagocytosis (Fig. 1B,C). She met HLH criteria and was started on HLH-94 protocol; however, her total and direct bilirubin climbed dramatically, peaking at 95.2 and 82.0 mg/dl, respectively. Rux 5mg BID was initiated as salvage therapy, and within 48 hours, her labs significantly improved, her fevers resolved, and she became responsive to blood transfusions (Fig. 1A). After two weeks on rux, she developed recurrent hemolysis. Her dose was increased to 20mg BID, resulting in a complete resolution of her hemolysis, fevers, transaminitis and hyperbilirubinemia. After 3 months of clinical stability, rux was tapered. She has been off rux now for three months.
Case 2: Patient 2 is a 26 yo woman who presented with unremitting fevers and myalgias, and was found to have an acute hepatitis C infection. Her ferritin was 24,023ng/ml, and a bone marrow biopsy demonstrated abundant hemophagocytosis. She initially responded to the HLH-94 protocol; however, attempts to hold treatment following induction were met with recurrent fevers, encephalopathy, and hyperferritinemia. She transferred to us, and a repeat bone marrow biopsy demonstrated persistent hemophagocytosis (Fig. 2B,C), while her ferritin was 15,073 ng/ml. We initiated salvage treatment with rux 10mg BID. Her fevers, encephalopathy, and lab abnormalities quickly improved; her ferritin fell to 2,973ng/ml within 3 days (Fig. 2A). A small subsequent elevation in her ferritin prompted an increase of the rux to 20mg BID. She improved and was discharged on rux maintenance at 20mg BID. Since discharge, she remains asymptomatic with mildly elevated ferritin levels, mild pancytopenia, and is tolerating a slow wean of rux without incident.
Case 3: Patient 3 is a 40 yo man with a diagnosis of hairy cell leukemia who received 5 days of cladribine. He developed febrile neutropenia 2 days following the end of chemotherapy. His infectious workup was negative with the exception of a positive peripheral blood EBV DNA PCR. He developed a mononucleosis-like syndrome, with persistent high fevers, splenomegaly, and hyperferritinemia to 6684 ng/ml. He also developed hepatic dysfunction with a direct hyperbilirubinemia peaking at 14.1 mg/dl and coagulopathy. He was treated initially with dexamethasone without resolution. A bone marrow biopsy demonstrated abundant hemophagocytosis (Fig. 3B,C). Given modest manifestations and concern that chemotherapy would exacerbate his immunosuppression, rux was initiated at 10mg BID. The liver dysfunction rapidly improved, and fevers resolved within 3 days (Fig. 3A). All other manifestations resolved within 1 week, and he was able to taper and discontinue rux within 2 months.
Conclusions: The preclinical data by Albeituni et al. coupled with our clinical observations suggest that ruxolitinib may be a viable alternative to aggressive chemotherapy regimens such as HLH-94 or anti-IFN-γ (emapalumab-lzsg) therapy for HLH, and clinical trials should be considered.
DiPersio:Karyopharm Therapeutics: Consultancy; Cellworks Group, Inc.: Membership on an entity's Board of Directors or advisory committees; NeoImmune Tech: Research Funding; Macrogenics: Research Funding, Speakers Bureau; Bioline Rx: Research Funding, Speakers Bureau; RiverVest Venture Partners Arch Oncology: Consultancy, Membership on an entity's Board of Directors or advisory committees; Magenta Therapeutics: Equity Ownership; WUGEN: Equity Ownership, Patents & Royalties, Research Funding; Amphivena Therapeutics: Consultancy, Research Funding; Incyte: Consultancy, Research Funding; Celgene: Consultancy.
Ruxolitinib was used off-label for the treatment of Hemophagocytic Lymphohistiocytosis (HLH) in the relapsed/refractory setting and in a patient who was unable to tolerate standard therapy. This was not in a clinical trial, but reported as a case series

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal