

Background: T cells are key players in immunotherapy but our understanding of their role and function in AML is limited. We have previously shown that following induction chemotherapy, the phenotypic and transcriptional profiles of peripheral blood (PB) CD8+ T cells in AML diverge between complete responders (CR) and non-responders (NR) to treatment (Knaus et al, JCI insight 2018). Further defining AML-induced T cell dysfunction is critical for immune monitoring and developing novel immunotherapeutic strategies.
Aims: 1. To characterize transcriptional differences between PB vs BM T cells of AML patients, similar to concept of circulating vs tumor infiltrating lymphocytes (TILs), and compare them to established immunologic signatures of solid tumors. 2. To examine the cumulative expression of multiple inhibitory receptors (IRs) on AML CD8+ T cells and their dynamics in PB vs BM at diagnosis (PRE-treatment) and POST-induction chemotherapy.
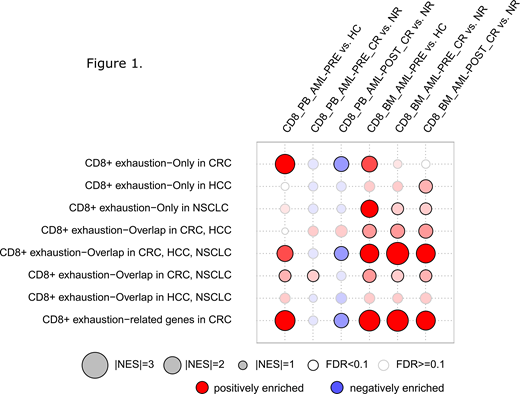
Methods: To study transcriptional signatures, we FACS-purified CD8+ T cells from BM of 6 AML patients (3 CR and 3 NR) PRE- and POST-induction chemotherapy whose PB T cells we analyzed and published previously (Knaus et al, JCI insight 2018). Samples were hybridized to the Human Prime View Gene Expression Array (Affymetrix). Expression fold change (FC), p-values and FDR were calculated. We compared our data set to those of dysfunctional T-cell signatures from non-small cell lung cancer (NSCLC: Guo et al, Nature 2018), colorectal cancer (CRC; Zhang et al, Nature 2018) and hepatocellular carcinoma (HCC; Zheng et al, Cell 2017) using gene set enrichment analyses (GSEA) and considered a normalized enrichment score NES>2 and FDR<0.1 as enriched.
Flow cytometry data on paired PB and BM samples from AML patients (n=32) PRE- and POST-treatment and healthy controls (HC; n=21) were used to calculate the IR-score (Thommen et al, Cancer Immunol Res 2015). The IR-score summarizes the cumulative relative amount of expression of 7 different IRs on CD8+ T cells. To determine the predictive ability of the IR score to differentiate CR from NR, Receiver Operating Characteristic (ROC) analysis was conducted using logistic regression, and the area under the ROC curve (AUC) was calculated.
Results: Immune signatures of AML CD8+ T cells at diagnosis, particularly in the BM, overlapped with transcriptomic exhaustion signatures of TILs from other malignancies (Figure 1-Overlap CRC, HCC, NSCLC), in particular that of CRC. Further, AML BM but not PB T cells showed a high enrichment for a common immune exhaustion signature shared by all 3 solid tumor entities and included IRs like HAVCR2, PDCD1, CTLA4, LAG3 and TIGIT, and other genes (e.g. TNFRSF9, CD27, IFNG, FASLG, CD39/ENTPD1) (Figure 1). Interestingly, this signature seemed to discriminate CR from NR patients only in the BM compartment, and at both PRE- and POST-treatment, thus providing a rationale for future exploration as a predictive biomarker of response.
We found that the flow-cytometry-based IR-score strongly discriminated between CR and NR in both the PB and the BM compartment POST-treatment with an AUC of 0.70 and 0.84, respectively. While IR-score including all 7 markers provided the best discriminatory value in the PB, the combination of only two senescence markers, CD57 and KLRG1, discriminated CR from NR patients in both PB and BM with an AUC of 0.69 and 0.79, respectively. The combination of 5 exhaustion markers (2B4, BTLA, Tim3, PD-1, and CD160) discriminated CR from NR patients only in the BM (AUC 0.79).
Conclusion: We found that in AML, T cells display a signature of immune exhaustion which is more prominent in the tumor milieu (e.g BM), similar to exhaustion signatures of solid cancers, can discriminate CR from NR, and persists in CR. Multiple genes, such as TNFRSF9, CD27, IFNG, FASLG, and CD39/ENTPD1, were higher expressed in CR patients both PRE and POST-treatment, suggesting that this signature also includes genes that could be useful for discriminating less dysfunctional T cell states. The phenotypic IR score was increased only in NR POST-treatment, indicating that assessment of a limited number of phenotypic markers may not be sufficient to address overall changes within T cells. Further exploration of AML-imposed T cell dysfunction is ongoing to inform better integration of immune-based therapies to augment anti-leukemia immunity.
Zeidner:Celgene: Consultancy, Honoraria, Research Funding; Daiichi Sankyo: Honoraria; Tolero: Honoraria, Research Funding; Pfizer: Honoraria; AsystBio Laboratories: Consultancy; Merck: Research Funding; Takeda: Research Funding; AbbVie: Honoraria; Agios: Honoraria. Gojo:Jazz: Consultancy, Honoraria; Novartis: Consultancy, Honoraria; Abbvie: Consultancy, Honoraria; Merck: Research Funding; Juno: Research Funding; Amgen Inc: Consultancy, Honoraria, Research Funding; Amphivena: Research Funding. Luznik:Merck: Research Funding, Speakers Bureau; Genentech: Research Funding; AbbVie: Consultancy; WindMiL Therapeutics: Patents & Royalties: Patent holder.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal