

The complex crosstalk between malignant chronic lymphocytic leukemia (CLL) cells and the tumor microenvironment (TME) is not fully understood. CLL is associated with an inflammatory TME and T cells exhibit exhaustion and multiple functional defects, fully recapitulated in Eµ-TCL1 (TCL1) mice and induced in healthy mice by adoptive transfer (AT) of murine CLL cells, making it an ideal model to test novel immunotherapies for this disease. Myeloid-derived suppressor cells (MDSCs), a non-leukemic cell type within the TME, are immature myeloid cells with the ability to suppress T cell function and promote Treg expansion. In humans, CLL cells can induce conversion of monocytes to MDSCs provoking their accumulation in peripheral blood (PB). MDSCs include two major subsets granulocytic (Gr) and monocytic (M)-MDSC. In mice, Gr-MDSCs are defined as CD11b+Ly6G+Ly6Clo and M-MDSC as CD11b+Ly6G-Ly6Chi. Both murine and human MDSCs express BTK. We observed that in CLL-bearing mice, MDSCs cells are lost in PB as disease progresses. Treatment with both BTK inhibitors (BTKi), ibrutinib (Ibr) and acalabrutinib (Acala), result in shift of T cell function from Th2 towards Th1 polarity and increase MDSC populations in vivo. We aimed to determine whether combination treatment with BTKi and chimeric antigen receptor (CAR) T cells renders recovery of the MDSC population in CLL-bearing mice.
To address this question we designed a two-part experiment, aiming to mimic the clinically relevant scenario of pre-treatment of CLL with BTKi to improve CAR T cell function. Part 1 of our experiment consisted of 4 groups (n=12) of 2.5 month old C57/Bl6 mice. Three groups had AT with 30x106 TCL1 splenocytes. A fourth group of WT mice remained CLL-free as a positive control and donors for WT T cells. When PB CLL load reached >10% (day 14) animals were randomized to either Ibr or Acala at 0.15 mg/l in 2% HPBC or no treatment for 21 days. All animals from part 1 were culled at day 35 post-AT and splenic cells were isolated, analyzed and used to manufacture CAR T cells. WT, CLL, Ibr and Acala treated T cells were activated and transduced with a CD19-CD28 CAR to treat mice in part 2. Here, 50 WT mice were given AT with 20x106 TCL1 splenocytes for CLL engraftment. All mice were injected with lymphodepleting cyclophosphamide (100mg/kg IP) one day prior to IV CAR injection. At day 21 post-AT, mice were treated with WT CAR, CLL CAR, IbrCAR, AcalaCAR or untransduced T cells. MDSC sub-populations were monitored weekly in PB and SP were analysed by flow cytometry.
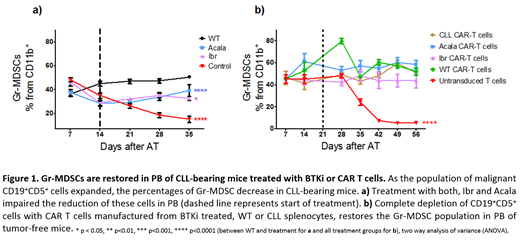
As malignant CD19+CD5+ cells expands in PB, the overall myeloid (CD19-CD11b+) cell population was not affected, but MDSCs significantly decreased (p<0.0001). Treatment with Acala, but not Ibr restores total MDSCs. However, MDSC impairment occurs in the Gr- but not M- MDSC population and both Acala and Ibr restores this population (Figure 1a). When we examined the spleen, treatment with both Ibr (p<0.001) and Acala (p<0.001) reduced CD5+CD19+ cells, whereas neither BTKi affected the overall myeloid (CD19-CD11b+) cell population. Gr-MDSCs were restored by both treatments whilst M-MDSCs were only restored after Ibr treatment (p<0.001 in each case). In part 2 of this experiment we observed that treatment with all CAR-T cell groups provokes the clearance of all CD19+CD5+ cells. The overall CD19-CD11b+ population stays the same across all mice groups 35 days after treatment in PB with any group of CAR and untransduced T cells. Overall MDSC population is maintained following all CAR T cells compared to CLL-bearing mice (p<0.0001) and it is the Gr- but not the M- MDSC population which is recovered in PB (Figure 1b). These parts of the experiments can of course be influenced by treatment with cyclophosphamide.
We conclude that novel therapies for CLL treatment have an effect not only in CLL cells but also in non-malignant cell components of the TME. In this animal model of CLL, the rapid expansion of CLL cells in PB and secondary lymphoid organs provokes loss of MDSC, particularly the Gr-MDSC subpopulation is affected. Treatment with BTKi and CAR T cells provokes clearance of CLL cells in PB and spleen allowing MDSC recovery; suggesting this may be BTK and ITK independent. We continue to explore secondary lymphoid organs to further characterize the shift of the CLL microenvironment from an immunosuppressive to an immune effective one and its impact on immune function in this model.
Sanderson:Kite/Gilead: Honoraria. Gribben:Celgene: Consultancy, Honoraria, Research Funding; Janssen: Consultancy, Honoraria, Research Funding; Abbvie: Consultancy, Honoraria, Research Funding; Acerta/Astra Zeneca: Consultancy, Honoraria, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal