


Patients < 60 years with acute ischemic stroke (AIS) are commonly tested for thrombophilia. Underlying this practice is the perception that the stroke may be the result of a hypercoagulable state, especially when an alternative cause is not evident. Although certain conditions, such as antiphospholipid antibody syndrome (APS), can be associated with AIS and require anticoagulation, inherited thrombophilia, largely, is not a risk factor for AIS even in young adults with cryptogenic stroke, as supported by case-control and prospective observational studies. Moreover, testing in the acute phase of AIS may give erroneous results (i.e., increase of Factor 8 as an acute phase reactant), and increase health care costs.
To assess our institutional performance on this matter, we conducted a retrospective chart review of 104 patients, age 18-60 years, who were admitted for AIS to Memorial Hermann Hospitals at the Texas Medical Center between 11/2016 and 7/2018, and whose stroke was considered cryptogenic or of undetermined origin (i.e., more than one possible causes) after initial diagnostic evaluation.
Mean age at the time of event was 43 (range 20-58) years. There were 61 (59%) males. Fifty nine (57%) patients were White, 42 (40%) Black, 18 (17%) Hispanic, 2 (2%) Asian, and one (1%) of unknown race. Risk factors for AIS were: hypertension in 64 (61%) patients, diabetes in 26 (25%), smoking in 27 (26%), dyslipidemia in 32 (31%), prior AIS in 17 (16%), coronary artery disease in 4 (4%), and obesity in 10 (10%). None had known atrial fibrillation or other cardiac arrhythmia.
Thrombophilia testing (at least one test) was performed in 82 (79%) of the patients. In the vast majority (70 patients, 85%) of cases, such testing was done within 1-3 days of admission as part of the initial stroke evaluation.
A total of 752 tests were performed on the 82 patients, 56 (7%) of which were positive. Increased Factor 8 (F8) activity (i.e., ≥200%) was the commonest abnormality observed (31/58 patients tested, or 53%), followed by low protein S (PS) activity (13/77, 17%), Factor V Leiden (FVL) mutation (3/71, 4%), low antithrombin (AT) activity (3/73, 4%), elevated homocysteine (2/79, 3%), low protein C (PC) activity (1/76, 1%), and positive APL (1/251, 1%), while no prothrombin gene mutation was seen. All but one of F8, PS, and AT tests were performed in the acute phase of the stroke. The estimated annual cost for testing was $65000.
Forty-two (51%) of the 82 patients tested had at least one abnormal test. In 2/42 (5%) of these patients, repeat testing (i.e., PS activity, F8) was done at least a month later, which, however, did not confirm the abnormality. Forty-seven (45%) patients were seen in the Outpatient Neurology Clinic after their stroke, for a median follow up of 5 (0.2 - 24) months. In 54 (52%) patients the cause of stroke remained undetermined even after thorough evaluation. Sixteen (15%) patients had a patent foramen ovale (PFO).
Of all patients tested, thrombophilia was confirmed in three, i.e., two patients with heterozygous FVL mutation and one with known homozygous FVL mutation and a significant personal history of venous thromboses.
Only in one patient (1/82, 1%) management was changed taking into account the thrombophilia testing results: a 57 year old male with low PS activity (tested 3 months after the stroke) and a PFO not amenable to closure, for whom anticoagulation was started despite the lack of venous thromboembolism.
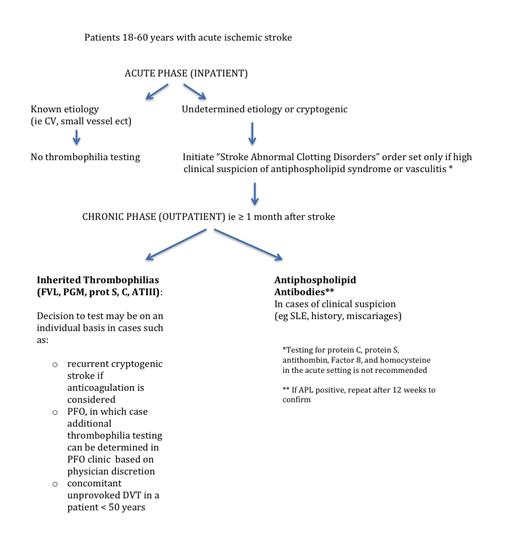
Based on these results, and due to concerns of indiscriminate testing, we created a practice guideline supported by current literature, as a reference for clinicians (see Figure). Briefly, we eliminated inherited thrombophilia testing in the acute phase, and rendered it optional in the chronic phase at the discretion of the treating physician, when anticoagulation is considered (i.e., some cases of PFO or recurrent stroke). Accordingly, we removed these tests from the admission order panel in the Electronic Medical Record. After internal audit and feedback from health care providers across disciplines, we submitted the new guideline for multidisciplinary review and system-wide adoption (i.e., multiple hospitals).
We conclude that routine thrombophilia testing is not an effective tool for secondary stroke prevention even in young patients with cryptogenic AIS. Institutional practice guidelines are helpful in tailoring such testing, hence avoiding misdiagnosis of a thrombophilic state and unnecessary costs.
No relevant conflicts of interest to declare.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal