

Introduction: The majority of published data about Deferasirox (DFX) are obtained on the dispersible formulation (DFX DT). A film-coated formulation (DFX FCT) with higher bioavailability is now approved and used in most countries, in tablets containing 30% less active principle. However, only few reports exist about long-term effects of DFX FCT and no independent comparison of the two formulations is available. Hypothesizing a bioavailability even higher than described, we conducted a study comparing PK/PD and safety of both formulations in a cohort of patients with congenital anemias.
Methods: Clinical records of patients treated at our referral Centre in the period from 2011 to March 2019 were reviewed, identifying patients that performed a 24-hours PK profile for both DFX formulations and completed at least 1 year of continuous treatment for each one. Data about PK (drug dose, maximum plasma concentration (Cmax), Area Under Curve (AUC)), PD (serum ferritin (FTN), Liver Iron Concentration (LIC) by biosusceptometry) and safety (ALT, AST, creatinine, eGFR, protein/creatinine ratio) were collected. Acute Kidney Injury (AKI) was defined according to guidelines as previously described (Bird, 2018). Estimated compliance was also considered. Serum DFX concentrations were measured by HPLC (De Francia et al, 2012). For PD and safety analysis, study time was defined as the period between two subsequent LIC measures; timeframes closest to the beginning of the therapy were selected. Wilcoxon matched-pairs test, Chi-square test and Spearman r index were used to analyze differences and correlations between DFX DT and DFX FCT treatments, with a significance threshold of 0.01.
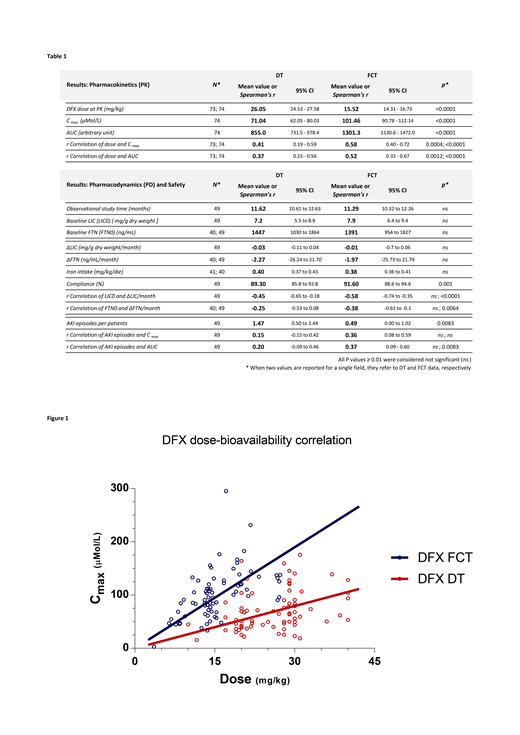
Results: Seventy-four patients diagnosed of β-thalassemia major (61), β-thalassemia intermedia (11), Diamond-Blackfan anemia (1) and Stomatocytosis (1) met inclusion criteria for PK analysis. DFX was tested at a mean dose of 26.1 (DT) and 15.5 mg/kg (FCT; -41%), with a Cmax of 71.0 and 101.5 μMol/L (+43%) and an AUC of 855.0 and 1301.3 (+52%), respectively. Cmax and AUC correlated significantly with dose for both formulation, but highly for FCT (r(dose-Cmax) = 0.41 and 0.58, r(dose-AUC) = 0.37 and 0.52 for DT and FCT, respectively), suggesting a stronger association between administered dose and systemic bioavailability (Fig.1). Forty-nine out of 74 patients, with at least 1-year follow-up for each formulation, were further analyzed for PD and safety. Actual administered dose was adjusted if indicated, but no significant differences were observed from doses tested at PK. LIC and FTN levels did not change significantly during treatments; as expected, the rate of iron overload variation (ΔLIC) was proportional to the iron overload at baseline for both formulations, but this correlation was stronger for FCT (Tab.1). Mean compliance was high with both formulations but improved significantly with DFX FCT (DT=89.3%; FCT=91.6%; p=0.001). Liver enzymes, creatinine, eGFR and protein/creatinine ratio at the end of treatments did not differ from baseline. AKI episodes were experienced in both formulations at rates comparable or higher than described (Diaz-Garcia, 2014 and Bird, 2018), but significantly lower with DFX FCT (DT=1.47; FCT=0.49 episodes/patient/year; p=0.0083). Overall kidney function was maintained at the end of the study for both treatments.
Discussion: This study presents a direct and extended comparison of DFX formulations from real-word experience. DFX FCT, even at doses lower than recommended (-41% instead of -30%) was superior to DT in terms of PK and comparable in overall PD after 1 year of observation. Here described for the first time, DFX FCT also resulted to be superior in terms of scalability, i.e. it showed better correspondence between administered dose and serum concentration and between the baseline iron burden and the rate of iron elimination during treatment. Acute renal impairment was confirmed to be a major complication of DFX treatment, however AKI prevalence was significantly lower for FCT and, consistently, a significant dose-dependent association was observed for FCT, but not DT. Altogether, our results suggest that FCT formulation is more bioavailable than expected and could improve chronic treatment with DFX, underlining the critical role of personalized dose tailoring and monitoring to maximize the delicate balance between effectiveness and safety .
Longo:Blue Bird Bio: Consultancy. Piga:Celgene Corporation: Consultancy, Research Funding; Novartis: Consultancy, Research Funding; Acceleron Pharma: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal