

Background:
Prophylactic treatment with replacement factor VIII (FVIII) is the standard of care for patients with severe hemophilia A to prevent bleeding and subsequent joint damage and chronic arthropathy. Because of variability in patient characteristics and clinical needs, it is recommended that prophylaxis is tailored to individual patient needs based on their baseline characteristics, bleeding history, and FVIII pharmacokinetic (PK) parameters. Endogenous levels of von Willebrand factor antigen (VWF:Ag) are known to influence the PK of FVIII. This analysis investigates the relationship between FVIII PK parameters and VWF:Ag levels, as well as between VWF:Ag levels and age, in patients with severe hemophilia A treated with various recombinant FVIII products using data obtained from multiple clinical trials.
Patients/Methods:
This integrated regression analysis is based on data with five FVIII products from six clinical trials. The products were: PEGylated recombinant FVIII BAY 94-9027 (damoctocog alfa pegol, Jivi®); sucrose-formulated recombinant FVIII (rFVIII-FS; Kogenate®-FS); BAY 79-4980 (liposomal version of Kogenate®-FS); unmodified full-length recombinant FVIII BAY 81-8973 (Kovaltry); and recombinant antihemophilic factor plasma/albumin-free method rAHF-PFM (octocog alfa, Advate®). The trials were: NCT01184820, NCT01029340, NCT00623727, NCT01233258, NCT02483208, and NCT01580293.
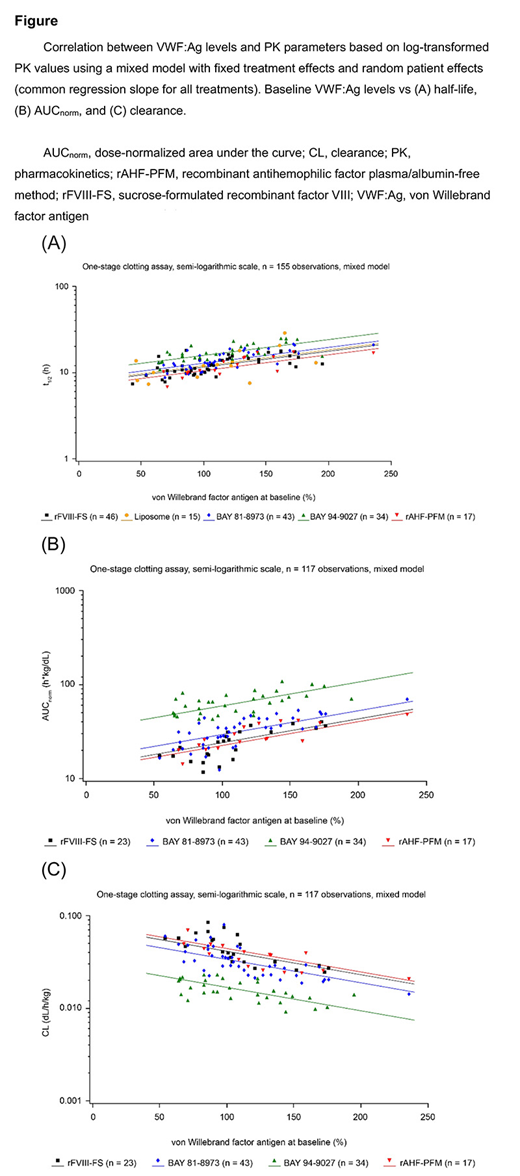
PK parameters were estimated by means of a non-compartmental analysis based on densely sampled single-dose profiles measured by one-stage and chromogenic assays, and following a dose of 25-60 IU/kg. The primary regression analysis was performed using the log-transformed PK parameters (half-life [t1/2], clearance [CL], and dose-normalized area under the curve [AUCnorm]) as dependent variables and the VWF:Ag levels as the independent variable in a mixed model including fixed treatment effects and random patient effects. In addition, the impact of age on VWF:Ag levels was investigated. One-stage assay results are reported. Results based on the chromogenic assay were in line with those reported for the one-stage assay.
Results:
Data from 104 patients from six studies were used to investigate the relationship of the dose-independent PK-parameter, t1/2 vs VWF:Ag levels, and of VWF:Ag levels vs age. Median age was 31 years (range 12-64 years). For the analyses of the PK parameters AUCnorm and CL, data from 77 patients from five studies were analyzed. Median age was 32 years (range 12-64 years). Some patients participated in multiple studies.
The primary regression analyses across all products and studies on the log-transformed PK parameters showed significant associations between PK parameters and VWF:Ag levels. Significant positive correlations vs VWF:Ag levels were observed for t1/2 (n = 155 observations in 104 patients, P < 0.001) and AUCnorm (n = 117 observations in 77 patients, P < 0.001), resulting in a negative correlation with CL (Figure 1). Other factors, such as age and the interaction of treatment with the VWF:Ag-PK effect, were found to be redundant and were not included in the final model.
Analysis of VWF:Ag levels vs age using a simple linear regression that did not incorporate the dependencies of multiple observations in patients, revealed a positive correlation between age and VWF:Ag levels (Spearman coefficient , r = 0.290 [P = 0.0029]; Pearson coefficient, r = 0.334 [P = 0.0005]). Comparable results were observed in a mixed model with random patient effects.
Conclusions:
In this combined analysis across five FVIII products, FVIII PK parameters (t1/2, AUCnorm, and CL) were significantly correlated with endogenous VWF:Ag levels which were also correlated with age. Moreover, while there were differences in the average PK parameters between products (represented by the intercept for treatment), all five FVIII products demonstrated similar VWF-PK relationships. It is well known that a patient's VWF:Ag level influences the PK of rFVIII, but this analysis suggests that the quantitative relationship between FVIII PK and VWF:Ag is similar for modified and unmodified FVIII products. This finding can be used, for example, to support selection of adequate treatment regimens when a patient is switching rFVIII product.
Maas Enriquez:Bayer: Employment. Delesen:Bayer: Employment. Solms:Bayer: Employment, Equity Ownership. Croteau:Novo Nordisk: Consultancy, Honoraria, Research Funding; Shire: Consultancy, Honoraria; Spark Therapeutics: Research Funding; Pfizer: Research Funding; Genentech: Consultancy, Honoraria; Octapharma: Honoraria; CSL Behring: Consultancy, Honoraria; Bayer: Consultancy, Honoraria. Berntorp:Bayer: Consultancy, Honoraria, Research Funding, Speakers Bureau; CSL Behring: Research Funding; Shire: Consultancy, Honoraria, Research Funding; Sobi/Bioverativ: Research Funding; Octapharma: Consultancy, Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal