

Introduction: The standard oral anticoagulant therapy administered to non-valvular AF patients has typically been Vitamin K Antagonists (VKA) particularly warfarin. In recent years, Direct Oral Anticoagulants (DOACs) including Direct Thrombin Inhibitors (DTI) and Direct Factor Xa inhibitors (FXa inhibitors) have become an alternative to warfarin. Randomized trials comparing warfarin and DOACs showed comparable effectiveness without significant additional major bleeding risk. However, bleeding events in RCTs may differ from those in daily use due to the routine exclusion of patients with a higher risk of bleeding from many studies. We aimed to assess bleeding risk between DOACs and warfarin in AF patients in observational studies and we also sought to determine differences between patients that were experienced or naïve to oral anticoagulants.
Methods: A systematic literature search was conducted in the OVID MEDLINE® and EMBASE® electronic databases. Observational studies and randomized control trials (RCT) from 1990 to January 2019 were retrieved and examined by two independent reviewers. A pooled effect hazard ratio (HR) was calculated using a random effects model using the generic inverse variance method. Subgroup analyses according to previous exposure to anticoagulants, study type, funding type and DOAC type were conducted. The primary outcome was major bleeding risk. The secondary outcome was clinically relevant non-major bleeding. All studies must have used an established or validated definition of major bleeding.
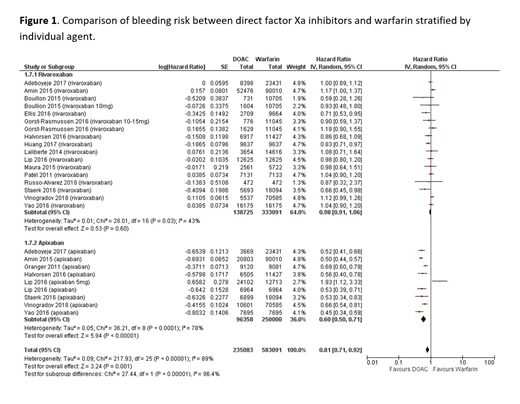
Results: The initial literature search identified 3359 potentially eligible citations. After primary screening, 150 articles were eligible for full text review and there were 35 studies including 2,356,201 patients that met the inclusion criteria. Overall, patients on DOACs were less likely to experience a bleeding event compared to warfarin (HR 0.78, 95%CI 0.71, 0.85, P<0.001). The results were consistent when analyzing patients receiving DTIs or FXa inhibitors (DTI: HR 0.76, 95% CI 0.67,0.87; FXa inhibitors: HR 0.79, 95% CI 0.69,0.89). However, among patients receiving factor Xa inhibitors, there was a significant difference in the risk of bleeding according to individual drug. Among patients receiving rivaroxaban the risk of bleeding was similar to warfarin (HR 0.98, 95%CI 0.91,1.06, p=0.60) whereas in those receiving apixaban there was a 40% reduction in the risk of bleeding compared to warfarin (HR 0.60, 95%CI 0.50,0.71, p<0.001) (Figure 1). Three studies reported information according to previous anticoagulant exposure. The overall pooled hazard ratio was 0.68 (95% CI 0.55, 0.82 p<0.001) in favor of patients on DOACs. In the subgroup analysis of previous anticoagulant use, the risk of bleeding was lower for DOACs compared to warfarin in both the experienced population (HR 0.70, 95%CI 0.51, 0.96) and the naïve population (HR 0.64, 95% CI 0.47,0.87). However, heterogeneity was moderate to high among both subgroups.
Conclusion: This review and meta-analysis of observational studies including over 2.3 million patients showed that overall DOACs have a lower risk of major bleeding and clinically relevant non-major bleeding compared to warfarin. Most importantly, although the pooled effect estimate did not differ between DTIs and FXa inhibitors, among patients receiving FXa inhibitors there was a significant difference between individual agents. Patients on apixaban had a significantly lower risk of bleeding compared to warfarin in contrast to patients on rivaroxaban who had a similar risk.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal