

Introduction
Cold agglutinin disease (CAD) is a rare autoimmune hemolytic anemia (AIHA) accounting for 20% of all cases, with no approved therapies and limited management options for patients. CAD is characterized by immunoglobulin M-mediated erythrocyte agglutination, which triggers activation of the classical complement pathway leading to hemolysis and subsequent anemia. Red blood cell (RBC) transfusions are used as a supportive treatment in CAD to temporarily alleviate anemia, although the transfusion practices are variable among providers treating patients with CAD. Recent RBC transfusion guidelines from the AABB (formerly the American Association of Blood Banks) recommend that transfusions be administered with a restrictive threshold in most clinical scenarios (ie, transfusion is not indicated until hemoglobin [Hb] reaches 7-8 g/dL and/or patients exhibit anemia-related symptoms) to avoid associated complications such as acute reactions, alloantibody development, and hemochromatosis (Carson et al, JAMA, 2016; Carson et al, N Engl J Med, 2017). Because of the dearth of information available regarding trends in RBC transfusion practices among US hematologists, the objective of this longitudinal, retrospective, observational assessment of an electronic medical record database was to evaluate transfusion practices applied to patients with CAD in the US.
Methods
Patients were retrospectively identified from Optum® de-identified Electronic Health Record (EHR) dataset. Adult patients with ≥1 AIHA-related medical encounter between January 2007 and September 2018 (study period) and ≥3 mentions of CAD-related terms from physician notes ("cold agglutinin disease," "cold autoimmune hemolytic anemia," or "cold agglutinin hemoglobinuria") were included (Broome et al, Blood, 2017).
The index date for each patient was the date of first mention of CAD during the study period. The baseline period was defined as the interval from the start of medical activity in the EHR database or study period (whichever occurred later) to the index date, and the follow-up period was defined as the interval from the index date to the end of the study period, end of medical activity, or death (whichever occurred earlier). The study sample was categorized into 2 study groups, the transfusion group (patients with CAD with ≥1 RBC transfusion after the index date) and the non-transfusion group (patients with CAD without any transfusions during the study period). Patients were further grouped based on the following Hb levels (g/dL): <8, ≥8 to ≤10, and >10 to ≤12. The closest Hb level prior to the most recent transfusion (within the prior 15 days and the lowest level) was used for the transfusion group and the lowest Hb level during the study period was used for the non-transfusion group.
Descriptive statistics included mean, standard deviation, and median values for continuous variables and frequency (n and percent) for categorical variables. No adjustment was made for this descriptive analysis.
Results
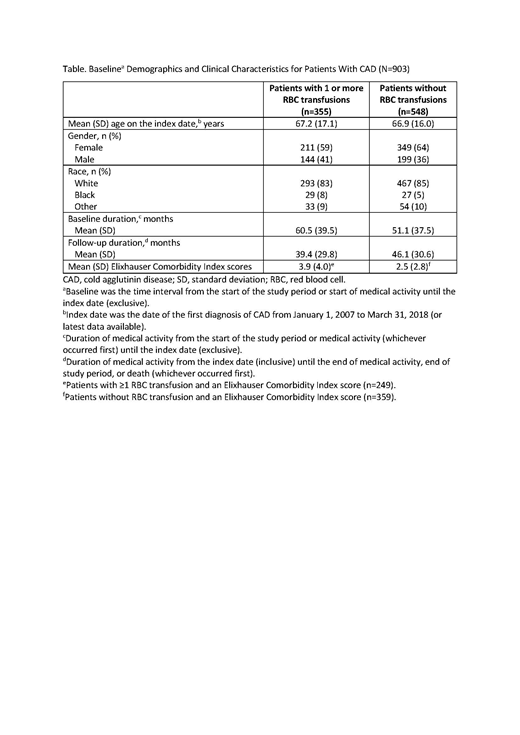
A total of 903 patients with CAD were identified from the Optum EHR database; most patients were white (n=760 [84%]) and female (n=560 [62%]). Baseline demographics and clinical characteristics of each group can be found in the Table.
Of the patients with CAD, 548 (61%) did not receive transfusions and 355 (39%) received ≥1 RBC transfusion. Among patients with CAD who received transfusions, 84% (n=297) had ≥2 RBC transfusions.
Out of the 903 patients with CAD, 864 had Hb levels reported and 752 had Hb levels ≤12 g/dL. Forty-four percent (n=329/752) of those CAD patients received ≥1 RBC transfusion. When separated by Hb levels, 18% of patients with Hb >10 to ≤12 g/dL (n=19/108); 41% (n=88/216) of patients with Hb ≥8 to ≤10 g/dL; and 52% (n=222/428) of patients with Hb <8 g/dL received ≥1 RBC transfusion.
Of the 423 (56%) patients with CAD and Hb levels ≤12 g/dL who did not receive RBC transfusions, 21% (n=89/423) had Hb levels >10 to ≤12 g/dL; 30% (n=128/423) had Hb levels ≥8 to ≤10 g/dL; and 49% (n=206/423) had Hb levels <8 g/dL.
Conclusions
Overall, patients with CAD are not a heavily transfused population. Even in those with a significantly decreased Hb (<8 g/dL), approximately half of them (49%) did not receive RBC transfusions. This suggests that the use of transfusions in patients with CAD may not reflect disease severity. Further prospective studies are needed to fully understand the impact of transfusions on patients with CAD.
Su:Sanofi Genzyme: Employment, Equity Ownership. Punekar:Sanofi: Employment, Equity Ownership. Morales Arias:Sanofi: Employment, Equity Ownership. Jain:Sanofi Genzyme: Employment, Equity Ownership.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal