

Background
Acute lymphoblastic leukemia (ALL) is frequent in Mexico, representing 51% of acute leukemia in adults. Hispanic ethnicity is associated with high-risk features and poor outcomes. We previously reported a multicenter experience in Mexico, where the majority of our ALL-patients (67%) were adolescents and young adults (AYA), mostly treated with HyperCVAD and with poor outcomes: 3-year overall survival (OS) of 25.7%. Many groups have demonstrated better outcomes with pediatric-inspired regimens (PIR) in the AYA-group, with long term OS > 60%. In 2016-2017 we changed the standard of care from HyperCVAD to PIR in two of the centers from the previously mentioned study.
Methods
We included AYA-patients with the diagnosis of Philadelphia-negative ALL treated with PIR (ALL-BFM 90 or CALGB 10403) between March 2016 and June 2019 in two centers in Mexico City. Both regimens were modified from the original: we used E. Coli asparaginase instead of pegaspargase and mercaptopurine instead of thioguanine. We compared these patients with our common historic database of patients with the same characteristics diagnosed between February 2009 and June 2015, treated with HyperCVAD. Hyperleukocytosis was defined as a white blood cell count > 30 x103/mcL for B-cell ALL and > 100 x103/mcL for T-cell ALL. Patients with t(v;11q23), hypodyploid or complex karyotype were considered high-risk. Baseline characteristics of both groups were compared with Chi-square or Mann-Whitney U test. We estimate OS by Kaplan-Meier method and compared groups by log-rank test. Multivariate Cox proportional hazards regression was used to evaluate independent prognostic factors associated with OS.
Results
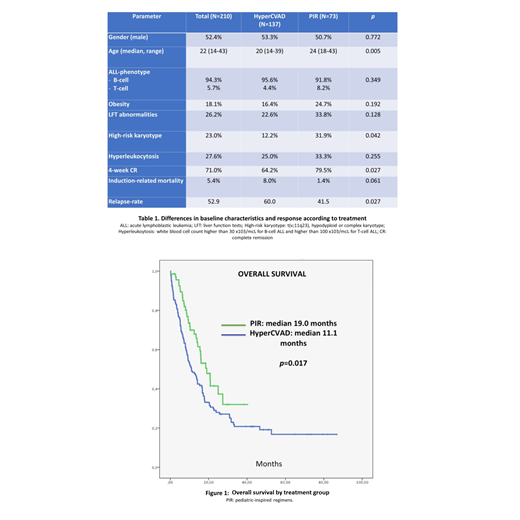
We compared 73 patients treated with PIR with a control group of 137 patients treated with HyperCVAD. The patients treated with PIR received either ALL-BFM 90 (N=46) or CALGB 10403(N=27). The median follow-up was 49.8, 23.3 and 12.7 months for HyperCVAD, ALL-BFM 90 and CALGB 10403 respectively. Patients treated with PIR were slightly older than those in the control group (median 24 vs. 20 years, p=0.005) and presented with high-risk karyotype more frequently (31.9% vs. 12.2%, p=0.042). Most of the patients were B-cell ALL (91.8% for PIR and 95.6% for HyperCVAD; p=0.349). Comparing PIR vs. HyperCVAD, there were no differences in the proportion of patients with hyperleukocytosis (33.3% vs. 25.0%, p=0.128) or obesity (24.7% vs. 16.4%, p=0.192). The induction related mortality was 5.7% for the entire group with a trend that favors PIR (1.4% vs. 8.0%, p=0.061).
In patients treated with PIR, the 4-week complete remission (CR) rate was higher (79.5% vs. 64.2%, p=0.027) and the relapse rate was lower (41.5% vs. 60.0%, p=0.027). Patients treated with PIR were more frequently treated with allogeneic stem-cell transplant (alloSCT) in first CR: 19.2% vs. 7.3%, p=0.017.
The median OS was significantly higher with PIR than with HyperCVAD, with a median of 19.0 months (3.3-25.4 months) vs. 11.1 months (7.3-14.8 months), and a 18-month OS of 53% vs. 33%, p=0.017.
When comparing the two different PIR (ALL-BFM 90 vs. CALGB 10403), the patients treated with ALL-BFM 90 had more frequently high-risk karyotypes (46% vs. 10.5%, p=0.012). Both regimens were associated with similar 4-week CR rate (78.3% vs. 81.5%, p=1). OS was higher with the CALGB 10403 with an 18 month-OS of 79% vs. 42% with the ALL-BFM 90 (p=0.044). When adjusted for high-risk karyotype, the benefit on OS was no longer significant.
In the multivariate analysis for OS, the independent significant prognostic factors were: treatment with a PIR (HR 0.428, 95% CI 0.221-0.826, p=0.011), alloSCT in first CR (HR 0.316, 95% CI 0.106-0.938, p=0.038) and high-risk karyotype (HR 2.695 95% CI 1.272-5.560, p=0.009).
Discussion
Although different groups have shown the benefit of PIR in the AYA-patients, the MD Anderson group couldn´t found any benefit from using the augmented BFM when compared to HyperCVAD. In our experience, the outcomes with HyperCVAD are poor in this group. In this report, the treatment with PIR was associated with a higher CR rate, lower relapse rate and better OS when compared with our historical HyperCVAD in AYA-patients. The benefit on survival was independent of other risk factors or alloHSCT. The main limitation of the study is the comparison with a historical group. However, given the general trend to treat these patients with RIP, a prospective randomized study in this regard is unlikely.
Demichelis:Abbvie: Speakers Bureau; AMGEN: Research Funding, Speakers Bureau; Celgene: Speakers Bureau; Novartis: Research Funding, Speakers Bureau; Shire: Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal