

Introduction:
T-cell lymphomas (TCL) are a heterogenous group of lymphoid malignancies that account for 10-15% of all lymphoproliferative disorders. Histological bone marrow involvement (BMI) ranges between 20-40% of all TCLs at time of diagnosis with bone marrow aspirate and biopsy (BMAB) considered the gold standard test to detect BMI. 18-Fluoro-deoxyglucose positron emission tomography combined with computed tomography (PET-CT) is a standard pretreatment imaging in the staging of TCL. In other lymphomas like DLBCL, PET-CT may obviate the need for BMAB as a component for staging, but this has not been studied in TCL. The aim of this retrospective study is to determine the accuracy of PET-CT in detecting BMI in newly diagnosed TCL.
Methods:
This is a single institution retrospective medical chart review study. All TCL patients(pts) diagnosed at Roswell Park Cancer Institute between January 2003 to December 2017 and underwent pre-treatment PET-CT and BMAB were included. PET-CT images were visually assessed for BMI. We excluded cases in which BMAB specimens were qualitatively and/or quantitatively insufficient to determine the presence or absence of BMI. Ann Arbor staging was determined using PET-CT and BMAB and the proportion of patients upstaged to Stage IV due to BMI detected by either modality was calculated. The BMAB and PET-CT results were summarized using a 2x2 contingency table. The performance of the PET-CT was evaluated using the sensitivity, specificity, positive predictive value, and negative predictive value. Confidence intervals for these measures were obtained using Jeffrey's prior method.
Results:
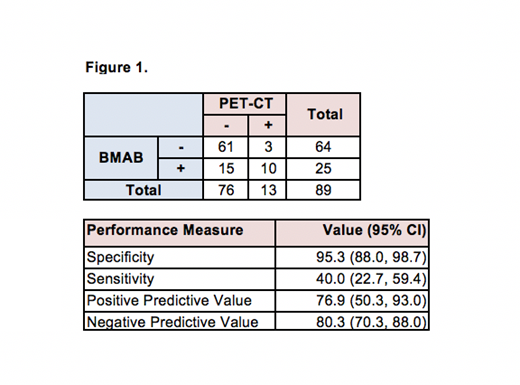
In total 89 pts were included in the analysis. Median age at time of diagnosis was 60 (range 20-92), 52 were male (58%), 20 had elevated LDH (22%), 7 had ECOG greater or equal to 2 (8%), 66 had an IPI score 0-2 (74%) and 23 had an IPI score 3-4 (26%), 7 had >2 extra-nodal sites of involvement (8%). In total, 38 pts (42.6%) had BMI at time of diagnosis, established by either BMAB (n= 25; 28%), PET-CT (n=13; 15%) or by both modalities (n=10 pts; 11%). There were 15 pts (17%) that were negative for BMI on PET-CT but had positive involvement of TCL on BMAB. The sensitivity and specificity of PET-CT to detect BMI by TCL was 40% (95% CI 22.7, 59.4) and 95.3% (95% CI 88.0, 98.7), respectively. Seventy-one pts (79.7%) had concordant results between lymphomatous BMAB and PET-CT (10 pts were positive for both, 61 pts were negative for both) and 18 pts (20.2%) had discordant interpretation (15 pts were negative by PET-CT and positive by BMAB and 3 pts were negative by BMAB and positive on PET-CT). BMAB upstaged 4 out of the 32 (12.5%) stage I-II pts to stage IV; out of these only 1 patient had positive BMI detected by PET-CT. The positive predictive value of PET-CT for detecting BMI was found to be 76.9 % (50.3, 93.0) with a negative predictive value of 80.3 % (70.3, 88.0) (Figure 1).
Conclusion:In our cohort of TCL pts, staging PET-CT does not identify all cases with BMI. BMAB upstaged more pts with Stage I/II to Stage IV than PET-CT. Although PET-CT has high negative predictive value for ruling out marrow involvement by TCL, BMAB remains a necessary component in the evaluation of pts with newly diagnosed TCL because of its ability to detect lymphomatous involvement of bone marrow missed by PET-CT which has implications in staging and treatment of TCL.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal