

Background: Ten to 15% of diffuse large B cell lymphoma (DLBCL) patients exhibit primary refractory disease (nonresponse or relapse within 3 months of therapy) and an additional 20-25% relapse following initial response. There is an unmet need for effective therapeutic regimens in relapsed/refractory (R/R) DLBCL. Lenalidomide is an immune modulator that reverses T cell dysfunction and also inhibits the NFκB pathway, which is constitutively active in non-germinal center (non-GCB) DLBCL. Lenalidomide and nivolumab, an anti-PD-1 antibody, each have single agent activity in R/R DLBCL. Here, we report the results of the dose-escalation cohort of this investigator-initiated, single-arm open-label study of the combination of nivolumab, lenalidomide and rituximab (NiLeRi) in R/R non-GCB DLBCL.
Methods: Adult patients with R/R non-GCB DLBCL, as determined by the Hans algorithm, with adequate organ function and an ECOG performance status of ≤2 were eligible for the study. The primary objective was to evaluate the safety of NiLeRi, and determine the maximum tolerated dose (MTD) of lenalidomide in combination with fixed doses of rituximab and nivolumab, using a 3+3 dose escalation design. The secondary objectives were to determine efficacy in terms of overall response rate (ORR), progression free survival (PFS), and overall survival (OS) of patients treated with NiLeRi. All patients received nivolumab IV 3 mg/kg on days 1 and 15 and rituximab IV 375mg/m2 on day 1 of each 28-day cycle. Lenalidomide was initiated at 5 mg po once daily on days 1-21. Additional planned dose levels were 10 mg, 15 mg and 20 mg. Patients were evaluable for toxicity if they received all doses of nivolumab and rituximab and at least 16 doses of lenalidomide during cycle 1 or if they experienced a dose limiting toxicity (DLT), regardless of the number of doses. NiLeRi was given for 8 cycles and patients with partial response could receive lenalidomide and nivolumab for an additional 4 cycles. Response was assessed by PET-CT after 2, 5 and 8 cycles and defined by Lugano criteria.
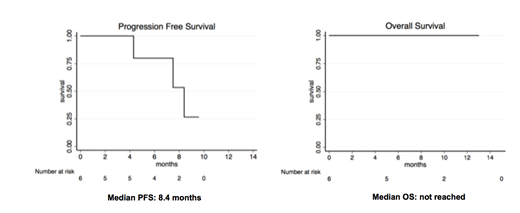
Results: Six patients with non-GCB subtype of DLBCL were enrolled in this study. The median age was 60.5 years (range 28-79), and 5 patients were male. The median number of prior lines of therapy was 4 (range 2-5), and the median IPI score was 3. None of the patients had bone marrow involvement. One patient each had been treated with autologous stem cell transplant (Auto-SCT) and CAR-T cell therapy. One patient withdrew consent before completing cycle 1 and was not evaluable for safety or efficacy. Safety: Five out of the six enrolled patients were evaluable for safety. All patients received lenalidomide 5 mg dose. Two patients experienced DLTs (grade 3 rash) resulting in lenalidomide discontinuation during cycle 2. The most common grade 3/4 toxicities were fatigue (20%), neutropenia (60%), thrombocytopenia (40%), and rash (40%). A total of 3 patients experienced grade 1/2 diarrhea and elevated liver enzymes. One patient experienced a grade 1 infusion reaction with rituximab. Efficacy: Patients who completed at least 1 cycle of therapy were evaluable for response, and this included 5 out of the 6 enrolled patients. The ORR and complete response (CR) rate were both 40%. Patients who responded did so early, with one patient achieving CR after 2 cycles and another patient achieving CR after 5 cycles. The best response seen in patients with primary refractory disease was PR. At a median follow up of 9.5 months, median PFS was 8.4 months (95% CI; 4.3 to not reached), and median OS was not reached.
Discussion: This is the first study reporting the safety results of the combination of lenalidomide, nivolumab and rituximab in non-Hodgkin lymphoma. Rash was the most common DLT, limiting dose escalation of lenalidomide above 5mg in this cohort of patients. Two patients experienced durable CR early in the study after 2 and 5 cycles, respectively. This ORR and CR rate of 40% each in this small cohort of patients who had relapsed after multiple prior lines of therapy is encouraging. Correlative studies, including whole exome sequencing of patient samples, are underway, in an attempt to explore predictive markers for response and toxicity.
Mason:Sysmex: Honoraria. Oluwole:Pfizer: Consultancy; Spectrum: Consultancy; Gilead Sciences: Consultancy; Bayer: Consultancy. Morgan:Biogen: Equity Ownership; Eli Lilly: Equity Ownership; Vertex: Equity Ownership; Zoetis: Equity Ownership; Pfizer: Equity Ownership; Novo Nordisk: Equity Ownership; Gilead: Equity Ownership; Johnson and Johnson: Equity Ownership; Merck: Equity Ownership. Reddy:Abbvie: Consultancy; Genentech: Research Funding; Celgene: Consultancy; BMS: Consultancy, Research Funding; KITE Pharma: Consultancy.
Nivolumab and lenalidomide are not FDA approved for use in diffuse large B cell lymphoma

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal