

Introduction
Malignancy can be heralded by unprovoked venous thromboembolism (VTE) but also by arterial thrombosis. To date it is unknown whether this association is present also in myeloproliferative neoplasms (MPN), in which arterial thrombosis is more frequent that venous thrombosis and solid tumors are reported with an increased frequency. The MPN-K nested case-control study addressed the impact of cytoreductive drugs on the risk of developing second cancer in MPN patients (Barbui T et al, Leukemia 2019); here we re-examined the study database to evaluate the frequency and type of vascular complications in MPN patients with second cancer excluding leukemia and to establish whether arterial and venous thrombosis during follow-up after diagnosis of MPN could predict the occurrence of a second cancer.
Patients and methods
Cases were patients with second cancer diagnosed concurrently or subsequent to the diagnosis of MPN. Controls were MPN patients without second cancer. For each case with second cancer, up to 3 cancer-free controls were matched by each center for sex, age at MPN diagnosis, date of MPN diagnosis, and MPN disease duration. Each set consisting of one case and their matched-controls had a similar observational period (from MPN diagnosis until the index date of diagnosis for the second cancer). The study included 647 cases with second cancer (carcinoma, non-melanoma-skin cancers, hematological secondary cancer and melanoma). The most frequent category was carcinoma (n=426, 65.8%). Cases were comparable with the 1,234 matched controls for demographics, type of MPN, and exposure to potential confounders such as mutational profile, abnormal karyotype and cardiovascular risk factors.
The thrombotic events of interest were ischemic stroke, transient ischemic attacks, acute coronary syndromes, peripheral arterial thrombosis, deep venous thrombosis (including thrombosis of cerebral and splanchnic veins) and pulmonary embolism. Thrombosis had to be concurrent with or in the 2 years before MPN diagnosis or occurring after MPN diagnosis.
The cumulative incidence of either arterial or venous thrombosis from MPN diagnosis was estimated by the Kaplan-Meier method and was compared between cases and controls using the log-rank test. A conditional logistic regression model estimated the Odds Ratio (OR) with 95% Confidence Interval (CI) of second cancer associated with the occurrence of thrombosis before/at diagnosis of MPN and during follow-up. Other covariates were patient age, cardiovascular risk factors, the JAK2V617F mutation, and treatment during follow-up.
Results
Approximately 20% of either MPN cases or controls had thrombosis before MPN or at diagnosis (19.8% vs. 21.1%, respectively, p=0.462). After a median observation time from diagnosis of MPN to an index date of 4.5 years (interquartile range 1.5-8.2) in cases and 3.7 years (interquartile range 1.5-7.5) in controls, cases showed a percentage of thrombosis higher than in controls (75/647, 11.6% vs. 100/1234, 8.1%, respectively, p=0.013). Approximately one-third of thrombosis preceding cancer occurred in the 12 months before the diagnosis of second cancer (22/75, 29.3%). The excess of thrombosis in cases was due to a higher frequency of arterial thrombosis (6.2% vs. 3.7%, p=0.015), whereas no significant difference was found for venous thrombosis (5.4% vs. 4.3%, p=0.277).
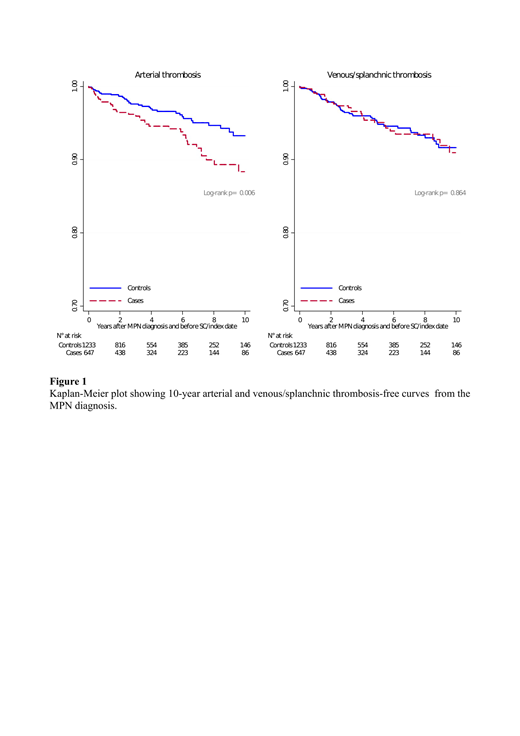
While the cumulative incidence of venous thrombosis over time was similar among cases and controls (p=0.864), the cumulative incidence of arterial thrombosis was higher in cases with second cancer (p=0.006) (Figure 1). The excess of arterial thrombosis after MPN diagnosis was limited to cases with carcinoma (6.8% vs 3.9%, p=0.027). In a multivariable model, arterial thrombosis during the follow-up was confirmed to be an independent predictor factor for carcinoma, with an odds ratio of 1.97 (95%CI 1.14-3.41, p=0.015).
Conclusions.
These findings reveal an association of arterial thrombosis with subsequent second cancer (namely carcinoma) in MPN patients. A possible biological plausibility for this link may be related to an underlying common pathogenic mechanism such as an aberrant inflammatory response consistently found in MPN. This observation may have practical implications and suggests careful clinical surveillance for early diagnosis of second cancer in MPN patients with arterial thrombosis during the follow-up.
Palandri:Novartis: Consultancy, Honoraria. Iurlo:Novartis: Other: Speaker Honoraria; Incyte: Other: Speaker Honoraria; Pfizer: Other: Speaker Honoraria. Bonifacio:Incyte: Honoraria; Novartis: Honoraria; Amgen: Honoraria; Pfizer: Honoraria; BMS: Honoraria. Rumi:novartis: Honoraria, Research Funding. Elli:Novartis: Membership on an entity's Board of Directors or advisory committees. Lunghi:Pfizer: Honoraria; Novartis: Honoraria; Incyte: Honoraria. Benevolo:Novartis Pharmaceuticals: Consultancy. McMullin:Italopharma: Membership on an entity's Board of Directors or advisory committees; Novartis: Honoraria, Speakers Bureau; Daiko Sanyo: Membership on an entity's Board of Directors or advisory committees. Griesshammer:Novartis: Consultancy, Honoraria, Speakers Bureau. Vannucchi:CTI: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Incyte: Membership on an entity's Board of Directors or advisory committees; Italfarmaco: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Celgene Corporation: Membership on an entity's Board of Directors or advisory committees. Rambaldi:Pfizer: Consultancy, Speakers Bureau; Novartis: Consultancy, Speakers Bureau; Celgene: Consultancy, Speakers Bureau; Amgen: Consultancy, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal