


The first two and last authors had an equal contribution.
Background: The Disease-Risk Index (Armand et al., Blood 2014) is an established system for risk stratification of patients undergoing allogeneic hematopoietic stem cell transplantation (HSCT). However, it was developed in patients transplanted approximately a decade ago, does not incorporate prognostic molecular data in acute myeloid leukemia (AML), and is not inclusive of several hematological malignancies. We sought to develop a contemporary risk-stratification scheme accounting for these limitations.
Methods: This retrospective study included adult patients treated for hematologic malignancies who underwent first allogeneic-HSCT between 2012 and 2016 in EBMT (European Society for Blood and Marrow Transplantation) centers. All donor types were included. Patients missing information on disease type, remission status, or survival data were excluded. Combinations of disease type and remission status were studied in a multivariable Cox-regression model for overall survival, adjusted for age, donor-type, cell source, donor/recipient sex disparity, and conditioning intensity. In de-novo AML and the myelodysplastic syndrome, cytogenetics were also integrated into the disease/remission status combinations. FLT3 and NPM1 mutational status were considered in de-novo AML patients in complete remission (CR). The risk model was developed on patients transplanted between 2012 to 2015 (training cohort). Temporal validation was performed on patients transplanted in 2016 (testing cohort). The DRSS was validated again on a cohort of patients transplanted between 2012 and 2016, in Italian centers reporting to the EBMT (validation cohort), who were excluded from the derivation or testing set.
Results: A total of 47,880 patients was studied. In the derivation cohort (n=33,943), the median age was 52 years. Indications for HSCT included acute leukemia (59%) followed by chronic myeloid malignancies (21%), lymphoma (16%), and plasma cell dyscrasia (4%). Unrelated donors were utilized in 57% of cases and HLA-matched related donors in 35%. Half of all patients received myeloablative conditioning. There were no clinically significant differences between the derivation and testing cohort (n=8,392), except an increase in Haplo-HSCT (5% to 9%, p<0.001). The validation cohort (n=5,545) was also similar to the derivation cohort with a high proportion of Haplo-HSCT (25%, [p<0.001]).
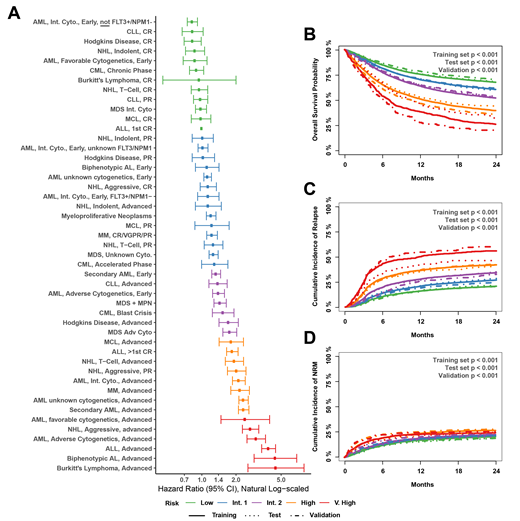
Combinations of disease and remission status were studied in a multivariable Cox-regression model developed on the training test (Figure 1A). We defined five risk groups based on a 33% increase in the hazard of mortality in each stratum. There was a monotonic increase in risk of mortality with each risk group in the derivation, test, and validation sets; the test set is presented here: low (HR=1), INT 1 (HR 1.20 [95% CI: 1.10-1.30]), INT 2 (HR 1.60 [1.43-1.79]), high (2.22 [1.99-2.47]), very high (2.81 [2.39-3.30]). On the test set, the low, intermediate 1, intermediate 2, high, and very high risk-groups had a 2-year overall-survival probability of 68%, 61%, 51%, 44%, and 31%, respectively (p<0.001) (Figure 1B); in the validation cohort, 2-year overall survival probabilities were similar: 70%, 62%, 54%, 36%, 20% (p<0.001). The decreasing survival was driven by a corresponding increase in 2-years relapse incidence (test: 22%, 28%, 34%, 40%, 48%, p<0.001; validation: 20%, 24%, 32%, 43%, 60%) (Figure 1C-D).
Conclusion: The DRSS is a contemporary risk stratification system for patients with hematological malignancies undergoing allogeneic-HSCT. The large cohort used to develop the system, along with temporal and geographical validation, suggest that the system is generalizable. Another advantage of the scheme is the incorporation of FLT3 and NPM1 in AML, the leading HSCT indication. DRSS should be used for risk stratification in statistical analyses, informed decision making, and planning of potential interventions across groups, including mixed indications for allogeneic-HSCT.
Labopin:Jazz Pharmaceuticals: Honoraria. Bug:Pfizer: Membership on an entity's Board of Directors or advisory committees; Jazz Pharmaceuticals: Honoraria; Hexal: Membership on an entity's Board of Directors or advisory committees; Gilead Sciences: Membership on an entity's Board of Directors or advisory committees, Other: Travel grants; Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: travel grants; Sanofi: Other: travel grants; Novartis: Membership on an entity's Board of Directors or advisory committees, Research Funding; Celgene Neovii: Other: travel grant. Mohty:Jazz Pharmaceuticals: Honoraria, Research Funding.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal