

Introduction: Abnormal metaphase cytogenetics are associated with inferior survival in newly diagnosed multiple myeloma (MM). These abnormalities are only detected in one third of cases due to the low proliferative rate of plasma cells. It is unknown if metaphase cytogenetics improve risk stratification when using contemporary prognostic models such as the revised international staging system (R-ISS), which incorporates interphase fluorescence in situ hybridization (FISH).
Aims: The aims of this study were to 1) characterize the association between abnormalities on metaphase cytogenetics and overall survival (OS) in newly diagnosed MM treated with novel agents and 2) evaluate whether the addition of metaphase cytogenetics to R-ISS, age, and plasma cell labeling index (PCLI) improves model discrimination with respect to OS.
Methods: We analyzed a retrospective cohort of 483 newly diagnosed MM patients treated with proteasome inhibitors (PI) and/or immunomodulators (IMID) who had metaphase cytogenetics performed prior to initiation of therapy. Abnormal metaphase cytogenetics were defined as MM specific abnormalities, while normal metaphase cytogenetics included constitutional cytogenetic variants, age-related Y chromosome loss, and normal metaphase karyotypes. Multivariable adjusted proportional hazards regression models were fit for the association between known prognostic factors and OS. Covariates associated with inferior OS on multivariable analysis included R-ISS stage, age ≥ 70, PCLI ≥ 2, and abnormal metaphase cytogenetics. We devised a risk scoring system weighted by their respective hazard ratios (R-ISS II +1, R-ISS III + 2, age ≥ 70 +2, PCLI ≥ 2 +1, metaphase cytogenetic abnormalities + 1). Low (LR), intermediate (IR), and high risk (HR) groups were established based on risk scores of 0-1, 2-3, and 4-5 in modeling without metaphase cytogenetics, and scores of 0-1, 2-3, and 4-6 in modeling incorporating metaphase cytogenetics, respectively. Survival estimates were calculated using the Kaplan-Meier method. Survival analysis was stratified by LR, IR, and HR groups in models 1) excluding metaphase cytogenetics 2) including metaphase cytogenetics and 3) including metaphase cytogenetics, with IR stratified by presence and absence of metaphase cytogenetic abnormalities. Survival estimates were compared between groups using the log-rank test. Harrell's C was used to compare the predictive power of risk modeling with and without metaphase cytogenetics.
Results: Median age at diagnosis was 66 (31-95), 281 patients (58%) were men, median follow up was 5.5 years (0.04-14.4), and median OS was 6.4 years (95% CI 5.7-6.8). Ninety-seven patients (20%) were R-ISS stage I, 318 (66%) stage II, and 68 (14%) stage III. One-hundred and fourteen patients (24%) had high-risk abnormalities by FISH, and 115 (24%) had abnormal metaphase cytogenetics. Three-hundred and thirteen patients (65%) received an IMID, 119 (25%) a PI, 51 (10%) received IMID and PI, and 137 (28%) underwent upfront autologous hematopoietic stem cell transplantation (ASCT). On multivariable analysis, R-ISS (HR 1.59, 95% CI 1.29-1.97, p < 0.001), age ≥ 70 (HR 2.32, 95% CI 1.83-2.93, p < 0.001), PCLI ≥ 2, (HR 1.52, 95% CI 1.16-2.00, p=0.002) and abnormalities on metaphase cytogenetics (HR 1.35, 95% CI 1.05-1.75, p=0.019) were associated with inferior OS.
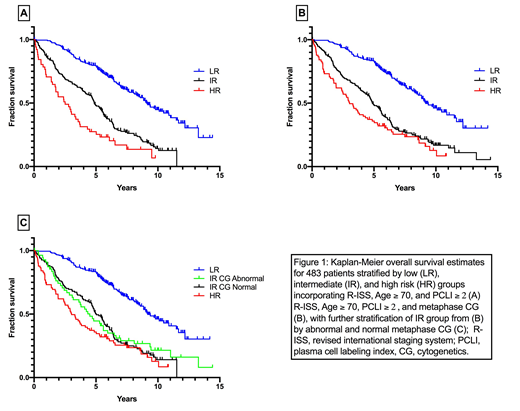
IR and HR groups experienced significantly worse survival compared to LR groups in models excluding (Figure 1A) and including (Figure 1B) the effect of metaphase cytogenetics (p < 0.001 for all comparisons). However, the inclusion of metaphase cytogenetics did not improve discrimination. Likewise, subgroup analysis of IR patients by the presence or absence of metaphase cytogenetic abnormalities did not improve risk stratification (Figure 1C) (p < 0.001).
The addition of metaphase cytogenetics to risk modeling with R-ISS stage, age ≥ 70, and PCLI ≥ 2 did not improve prognostic performance when evaluated by Harrell's C (c=0.636 without cytogenetics, c=0.642 with cytogenetics, absolute difference 0.005, 95% CI 0.002-0.012, p=0.142).
Conclusions: Abnormalities on metaphase cytogenetics at diagnosis are associated with inferior OS in MM when accounting for the effects of R-ISS, age, and PCLI. However, the addition of metaphase cytogenetics to prognostic modeling incorporating these covariates did not significantly improve risk stratification.
Lacy:Celgene: Research Funding. Dispenzieri:Akcea: Consultancy; Intellia: Consultancy; Alnylam: Research Funding; Celgene: Research Funding; Janssen: Consultancy; Pfizer: Research Funding; Takeda: Research Funding. Kapoor:Celgene: Honoraria; Sanofi: Consultancy, Research Funding; Janssen: Research Funding; Cellectar: Consultancy; Takeda: Honoraria, Research Funding; Amgen: Research Funding; Glaxo Smith Kline: Research Funding. Leung:Prothena: Membership on an entity's Board of Directors or advisory committees; Takeda: Research Funding; Omeros: Research Funding; Aduro: Membership on an entity's Board of Directors or advisory committees. Kumar:Celgene: Consultancy, Research Funding; Janssen: Consultancy, Research Funding; Takeda: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal