

Background: Allogeneic stem cell transplant (allo-SCT) is a cornerstone in the treatment of Acute Myeloid Leukemia (AML) exerting much of its therapeutic efficacy through the graft-versus-leukemia effect. The administration of immunoregulatory cells via engrafted donor lymphocytes is essential to the eradication of residual malignancy and long-term survival. Many patients, however, either do not have an allo-SCT donor or cannot withstand the toxicity of allo-SCT.
Previous studies have shown durable responses in AML patients following donor lymphocyte infusions in the absence of engraftment in both the frontline and relapsed setting (Dey et al, BJH 2005, Colvin et al, BBMT 2009, Ai et al, Blood 2010). In this clinical trial we propose a role for donor leukocyte infusions (DLI) in the absence of engraftment. Without the need for engraftment patients will not need to receive high dose chemotherapy or radiation and the toxicities that accompany these therapies. Instead, allogeneic donor cells are infused into patient with relapsed/refractory (R/R) AML to serve as a potent immune stimulator.
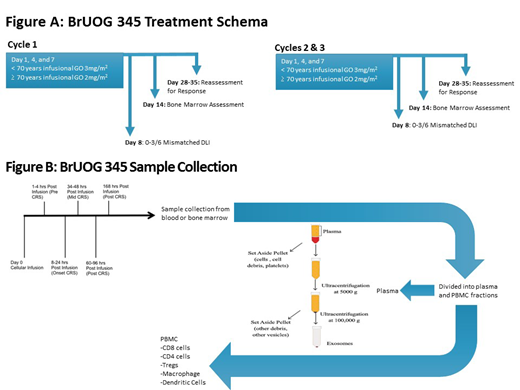
Prior to DLI, patients will receive fractionated dosing of gemtuzumab ozogamicin (GO). GO is an anti-CD-33 antibody drug conjugate approved in combination with induction therapy for de novo AML and in R/R disease. Patients who demonstrate a CR or CRi to therapy will go on to have up to 2 additional GO + DLI treatments. Bone marrow and blood samples will be obtained from patients before, during, and after treatment to determine immune effector cells (both donor and patient), cytokine release profiles, and extracellular vesicle components.
Study Design and Methods: Our study, BrUOG 345 [NCT03374332], evaluates the combination of fractionated GO with non-engraftment DLI in the treatment of patients with R/R AML. Adults patients 18 years of age and older with histologically confirmed R/R AML who have had recurrence or progression after at least 1 prior standard treatment are eligible. Enrollees must have no active systemic infections and have adequate lung, liver, cardiac, and renal function with an ECOG PS 0-1. Fractionated GO 6-9mg/m2 will be administered on days 1, 4, and 7 followed by infusion of 1-2x108 CD3 cells/kg from a 0-3/6 HLA mismatched related donor cell. Patients that are in CR or CRi can receive up to 2 additional treatments with GO+DLI (Figure 1).
The primary objective of the phase 1 portion is to determine the maximum tolerated dose (MTD) of DLI in combination with GO while the primary objective of Phase 2 portion is to assess the response rate after one cycle of fractionated GO followed by non-engraftment DLI in patients with relapsed/refractory AML. The study will initially utilize a 3+3 design in Phase 1 to determine if 1-2x108 CD3 cells/kg can be safely administered with GO.
This study will target a response rate of 57% considered to be interesting enough to warrant further study in a randomized setting. With this hypothesis in mind, the phase 2 portion of the study will use Simon's two-stage design. The null hypothesis that the true response rate (CR and CRi) is only 29% will be tested against a one-sided alternative. In the first stage, 9 subjects will be accrued. Patients treated at MTD in the Phase 1 portion of the study will be included in this cohort. If there are 3 or fewer responses in these 9 patients, the study will be stopped for futility. Otherwise, 6 additional subjects will be accrued for a total of 15. The null hypothesis will be rejected if 7 or more responses are observed in 15 patients. This design yields a type I error rate of 0.1 and power of 80% if the true response rate is 57%.
A continuous assessment of toxicity will be utilized for the Phase 2 portion of this study. Sequential boundaries will be used to monitor dose-limiting toxicity rate for patients after the initial MTD is determined. Accrual will be halted if excessive numbers of dose-limiting toxicities are seen.
The primary outcome of the Phase 2 portion is the CR/CRi rate following GO and non-engraftment DLI. Secondary outcomes will include survival, both progression-free (PFS) and overall (OS) until two years post treatment, and dose limiting toxicities until 16 weeks post-infusion. Additional lab correlative studies will be performed including CD33 expression before, during, and after GO infusion and T-cell activation markers, antigen presenting cell/macrophage amounts, cytokine release profiles, and extracellular vesicle measurements (Figure 1).
Olszewski:TG Therapeutics: Research Funding; Spectrum Pharmaceuticals: Research Funding; Adaptive Biotechnologies: Research Funding; Genentech: Research Funding. Reagan:Pfizer: Research Funding; Incyte: Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal