

Background:
Cytomegalovirus (CMV) reactivations are common post allogeneic stem cell transplant (ASCT) especially in developing countries like India, where most of the patients as well as donors are CMV seropositive. Ganciclovir is the drug of choice for preemptive therapy. However, myelosuppression which is a prominent side effect of ganciclovir, precludes its use in many post ASCT patients who are already cytopenic. Unavailability of second line agents like foscarnet and cidofovir in India leaves few therapeutic options for such patients. Artesunate is an inexpensive antimalarial agent and has been sporadically reported in literature to be effective in CMV reactivation in patients who are intolerant or resistant to ganciclovir. Here we report utility of artesunate in ASCT patients who could not be given or continued on ganciclovir due to cytopenias. This is the largest report of artesunate use in CMV reactivation to the best of our knowledge.
Methods:
All patients who underwent ASCT between April 2015 and October 2018 were included in this retrospective analysis. CMV IgG serology was tested at baseline for patients and donors. Conditioning regimen used was either myeloablative (CyTBI/BuCy) or reduced intensity with fludarabine in combination with either melphalan or treosulphan + 2 Gy TBI. Graft versus host disease (GVHD) prophylaxis used was calcineurin inhibitor (CNI), with methotrexate or mycofenolate mofetil (MMF) for matched sibling (MSD) and matched unrelated donor (MUD) transplants. MUD transplant recipients additionally received rabbit ATG (2.5-5 mg/kg). Post transplant cyclophosphamide (PTCy) with CNI and MMF was used for haploidentical transplants (HIT).
CMV was monitored twice a week with quantitative polymerase chain reaction (QPCR) from start of conditioning till at least D+100 post ASCT or longer if patient was on immunosuppression. Those with a QPCR >500 copies/mL at 2 consecutive time points were started on preemptive therapy. Ganciclovir was preferred as first line agent, however in case of cytopenia, artesunate was used. In case cytopenia developed while patient was on ganciclovir, artesunate was started as second line. Artesunate dose was 2.4 mg/kg (upto 120 mg) twice daily. Artesunate was given till clearance of CMV (unquantifiable CMV DNA on QPCR at 2 consecutive time points) or intolerance. Artesunate failure was defined as > 1 log increase in CMV copies after 2 weeks of therapy or development of CMV end organ involvement while on therapy. Artesunate was considered to be effective if there was no log increase in CMV copy numbers at 2 weeks of therapy. Biopsies from relevant organs were performed to detect CMV disease, when clinically indicated.
Results:
One hundred and seventeen patients underwent ASCT in this period. There were 73 MSD, 34 HIT, 7 MUD, 3 mismatched sibling donor (MMSD) transplants. There were 78 episodes of CMV reactivation in 69 patients (58%). Incidence was highest in HIT -73% followed by MMSD - 66%, MUD- 57% and MSD - 43%.
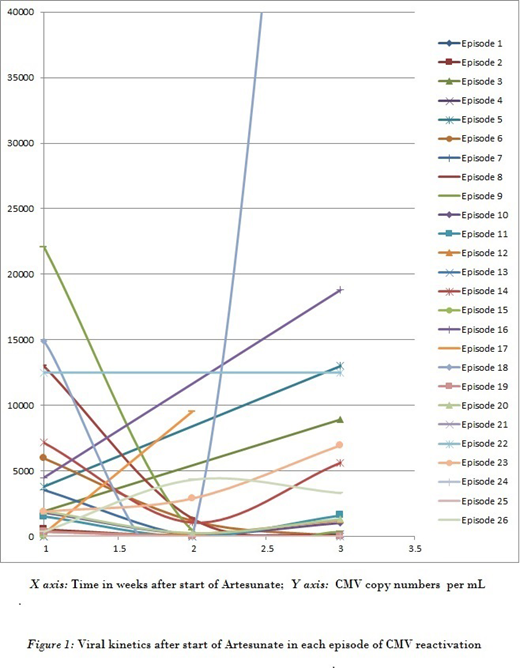
Artesunate was used in 25 patients for 27 (34%) of the total 78 episodes; as 1st line agent in 6, 2nd line in 13 and 3rd line in 8 episodes. Median CMV viral load was 1.6x 103 copies per mL at start of artesunate. Median duration of use was 14 days (range 6 to 49). It was used preemptively in 15 episodes and as therapeutic (end organ involvement) in 12. Five (19%) of the 27 CMV episodes cleared with artesunate. However artesunate was effective in controlling CMV proliferation (absence of log increase in CMV copy numbers at 2 weeks and absence of progression to end organ CMV disease) in 20(74%) of 27 episodes.Artesunate failure rate was 22% (6 of 27 episodes). Response could not be evaluated in 1 patient. The CMV kinetics of the 26 episodes is depicted in figure 1. Twenty two patients tolerated artesunate with no major toxicities. However, 3 patients developed haemolysis likely artesunate related, requiring stoppage of the drug.
Conclusions:
Artesunate has activity against CMV with failure rate of less than 25% and complete clearance in 20%. In resource limited settings, it may be used in patients who are cytopenic and intolerant to ganciclovir as it limits proliferation of CMV which was seen in about 3/4th of all episodes. Its role in CMV infection should be explored prospectively in settings where ganciclovir cannot be used and access to other CMV active drugs are limited.
Artesunate is an antimalarial drug which has been used for CMV reactivation in this study

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal