

Introduction: The shift toward long-term, targeted therapies for patients with CLL requires fit-for-purpose patient-reported outcome instruments (PROs) to assess overall treatment benefit. The FACIT-Fatigue is designed to assess fatigue-related symptoms and their impact on daily functioning, with extensive published evidence of its reliability and validity in cancer populations, although not specifically for CLL. This study evaluates the psychometric properties of the FACIT-Fatigue in patients with relapsed or refractory CLL to determine if it is fit-for-purpose in this population.
Methods: Data were from baseline assessments in a multicenter, open-label, phase 3 study that enrolled patients with relapsed or refractory CLL (ClinicalTrials.gov Identifier: NCT02970318). Patients completed the following PROs at baseline: FACIT-Fatigue; European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-Core 30-questions (EORTC QLQ-C30); and EuroQol 5-Dimension 5-Level instrument (EQ-5D-5L), including its global health visual analog scale (EQ-VAS). The FACIT-Fatigue includes a 5-item symptom scale (Sx) and an 8-item impact scale (Imp) that together make up the 13-item Total score. Item responses range from 0 ("not at all") to 4 ("very much"). Scores for negatively worded items are reversed, such that higher scores are better (i.e. less fatigue). The EORTC QLQ-C30 contains 8 multi-item function (Physical, Role, Cognitive, Emotional, Social) and symptom (Fatigue, Pain, Nausea/Vomiting) scales, 5 single-item symptom scales (Dyspnea, Insomnia, Appetite Loss, Constipation, Diarrhea), a Global Health Status scale and a single-item financial impact scale. The EQ-5D-5L comprises five impairment-related dimensions (Mobility, Self-care, Usual Activities, Pain/Discomfort, Anxiety/Depression). EQ-VAS is a 0-100 scale of a patient's health status. FACIT-Fatigue psychometric assessments included descriptive statistics for items and scales, item-to-item and item-to-total analysis, internal consistency reliability and construct (convergent and known-groups) validity. Convergent validity was assessed based on correlations with the EORTC QLQ-C30 and EQ-VAS. Baseline known-groups were defined by Eastern Cooperative Oncology Group (ECOG) status (0 or 1 vs. 2), hemoglobin level (<110 g/L vs. ≥110 g/L) and constitutional symptoms (night sweats, fever, unexplained weight loss, significant fatigue [none vs. ≥1 symptom]). Cluster analysis (based on groupings by FACIT-Fatigue and EORTC QLQ-C30 scores) was performed to identify a FACIT-Fatigue severity cut-off score.
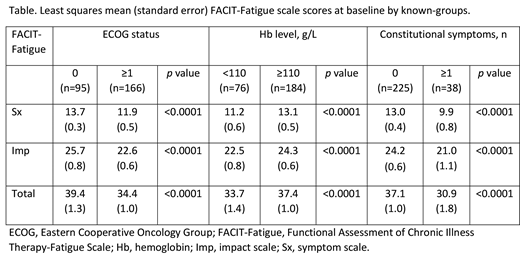
Results: Baseline PRO data were available for 263 patients. Mean scores ranged from 1.01 to 1.84 for Sx items and from 0.40 to 2.23 for Imp items. The proportion of patients answering "not at all" was >25% for 1 of 5 Sx items but for 7 of 8 Imp items, indicating that at baseline there was low impact of fatigue on activities. Most item-to-item correlations and all item-to-total correlations were moderate to strong (Spearman's rank correlation coefficient r≥0.3). The FACIT-Fatigue demonstrated good internal consistency reliability, with Cronbach's coefficient α of 0.87, 0.86 and 0.91 for the Sx, Imp and Total scores, respectively. Sx, Imp and Total scores correlated strongly with the EORTC QLQ-C30 Global Health Status, Physical Function, Role Function and Fatigue scale scores, and the EQ-5D-5L VAS score (all Spearman's r≥0.5), demonstrating convergent validity. Weak correlations (r≤0.3) were observed between the FACIT-Fatigue scales and the EORTC QLQ-C30 Insomnia, Constipation and Diarrhea scales, indicating that there is no relationship between fatigue and these symptoms, and demonstrating discriminant validity. Known-groups validity of the FACIT-Fatigue scales was demonstrated by significant differences between groups defined by baseline ECOG status, hemoglobin level, and constitutional symptoms (Table). Cluster analysis supported a FACIT-Fatigue Total score threshold of either 30 or 34 (Cohen's kappa coefficients of 0.76 and 0.67, respectively) to define a severe fatigue population.
Conclusions: Psychometric analyses in patients with relapsed or refractory CLL demonstrated that the FACIT-Fatigue has good psychometric properties and is fit-for-purpose in this population. Results support the use of the FACIT-Fatigue in these patients in the clinical trial setting.
Eek:AstraZeneca: Employment, Equity Ownership. Ivanescu:Astellas: Consultancy. Kool-Houweling:IQVIA: Employment. Cella:FACIT.org: Equity Ownership.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal