

Background: Myelodysplastic Syndromes (MDS) are a heterogeneous hematologic malignancy characterized by bone marrow failure and cytopenias. The median survival rate for patients with higher-risk MDS who fail standard-of-care chemotherapy with hypomethylating agents (HMAs) is less than 6 months, and the only curative treatment for these patients is hematopoietic stem cell transplant (HSCT). Over the past 10 years, immunotherapy as a cancer treatment has achieved variable levels of success in different tumor types. There are currently 22 active clinical trials of immunotherapies for MDS (www.clinicaltrials.gov; 7/30/19), including our phase I clinical trial with a personalized adoptive cellular therapy targeting MDS patient neoantigens (NCT 03258359). Because MDS patients are frequently monocytopenic and the existing literature is inconsistent regarding the ability of MDS patients' monocytes to support T cell activation, we compared the activation of MDS T cells with those of healthy donors in the presence of autologous monocytes.
Methods: Peripheral blood mononuclear cells (PBMC) from 5 healthy donors and 7 higher-risk MDS patients were cryopreserved after Ficoll separation. These PBMC were thawed and aliquoted into 6 replicate wells of 200,000 cells in 96-well u-bottom plates in R-10 culture medium. Half of the wells were treated with 25 ng/mL OKT3 and 200 U/mL IL-2. After 48 hours at 37˚C with 5% CO2, the wells were collected for analysis by flow cytometry. Beads were used to detect T cell activation induced secretion of IFNg, TNFa, IL-4, IL-10, and IL-17 in the supernatant and fluorescent antibodies were used to phenotype viable cells for CD3, CD4, CD8, and the T cell activation markers, CD69, CD25, CTLA-4, PD-1, and HLA-DR.
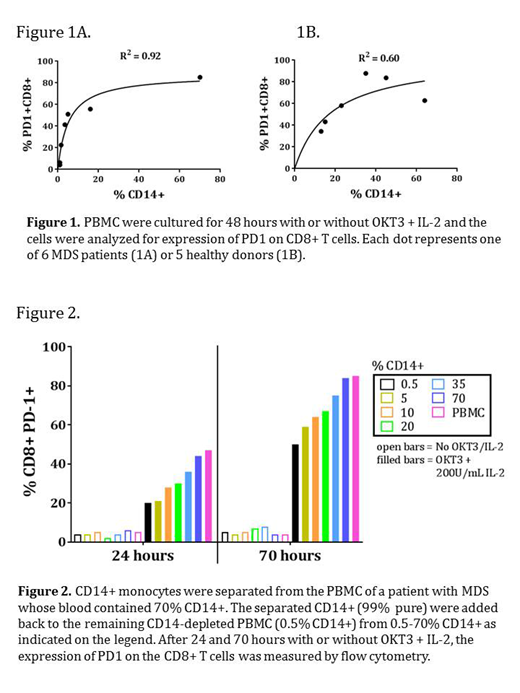
Results: We measured a higher release of IFNg and TNFa in donor PBMC compared to MDS patients after OKT3/IL-2 activation, p < 0.01 and 0.04, respectively by 2-way ANOVA. The expression of CD69, CD25, HLA-DR, and CTLA4 increased variably on activated T cells from donors or MDS patients, but expression of CD4+CD25+ was more frequent on donor T cells after activation (p = 0.03). Activation also resulted in a higher frequency of PD-1 expression on donor CD4+ and CD8+ T cells than on MDS T cells (p < 0.01 and < 0.01, respectively). Interestingly, on both MDS and normal T cells the percentage of CD8+PD1+ activated cells correlated strongly with the percent of CD14+ monocytes present in the PBMC (R2 = 0.92 and 0.60 respectively; Fig 1a and 1b). We designed further experiments to test whether this was a patient intrinsic phenomenon, or if the absolute number of CD14+ monocytes in the PBMC was associated with different levels of PD1 expression upon T cell activation. First, we separated CD14+ cells from the PBMC of a patient with MDS using magnetic beads. Then CD14+ cells were added back to the CD14-depleted PBMC at a final percent of 0.5, 5, 10, 20, 35, 70, or 100% of the original amount. Unmodified PBMC was included as a control and all cells were stimulated with OKT3 and IL-2 or left in R-10 medium without stimulus. After 24, 48, and 70 hours, samples were collected to analyze by flow cytometry for CD3, CD4, CD8, CD14, and PD1 expression. The results show that an increasing percent of monocytes corresponded to the increased expression of PD1 on CD8+ and CD4+ T cells.
Conclusion: Our results show that there are variable reductions in markers of T cell activation and cytokine secretion in MDS patients compared to healthy donors. We also observed that the fold increase in activation induced PD-1 expression was well correlated with the percent of CD14+ monocytes in the PBMC of both MDS patients and healthy donors. Direct experimentation revealed that this correlation is a cause-effect relationship. We are continuing to investigate the role of monocytes in T cell activation in MDS patients.
Bejar:Celgene: Consultancy; Takeda Pharmaceuticals: Research Funding; AbbVie/Genentech: Consultancy, Honoraria; Astex/Otsuka: Consultancy; Modus Outcomes: Consultancy; Daiichi-Sankyo: Consultancy. Lane:PersImmune, Inc.: Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal