

Introduction:
Catastrophic antiphospholipid syndrome (CAPS) is characterized by multiple intravascular thrombotic events occurring over a short time period in the presence of persistently detectable antiphospholipid antibodies (APLA). Despite its clinical significance with mortality rate of 40-50%, the underlying pathophysiology remains somewhat enigmatic. More recent focus on the complement system as it interacts with the coagulation cascade has led to off-label use of eculizumab, a humanized monoclonal antibody against C5, in the treatment of CAPS.
Consequently, monitoring of disease status with complement levels is an area of interest. We report complement levels in four patients with CAPS who had various clinical outcomes.
Methods:
Four patients admitted to SUNY Upstate Medical University with CAPS between February and May 2019 were included in this case series. All patients had APS with prior history of refractory CAPS (persistent disease despite standard therapy with steroids, rituximab, and therapeutic plasma exchange [TPEX]). Antiphospholipid antibodies (APLA) and complement (C3 and C4) levels were monitored during admission until discharge or death.
Results:
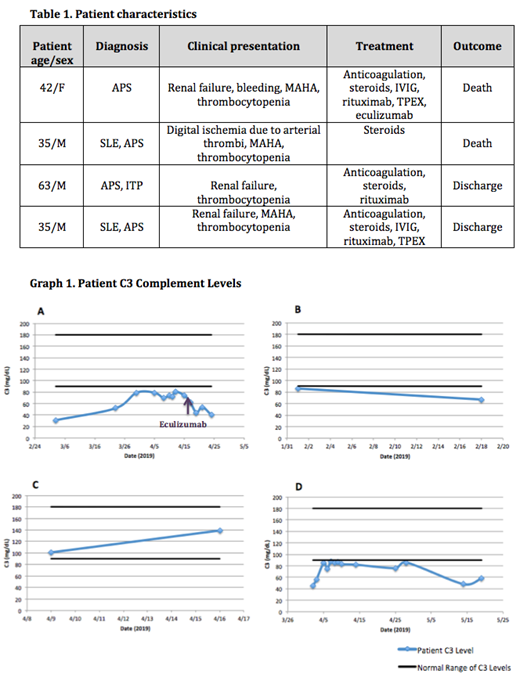
Patient characteristics are summarized in Table 1.
Patient 1 was a 42-year-old female with antiphospholipid syndrome (APS) on warfarin, ischemic stroke, and aortic valve replacement admitted on March 2019 with shortness of breath, hemoptysis and menorrhagia. She was found to have elevated APLA, thrombocytopenia, and acute renal failure with renal biopsy confirming APS nephropathy. Despite therapy with ongoing anticoagulation, steroids, rituximab, IVIG, and TPEX her clinical course continued to deteriorate. Hypocomplementemia was present (both low C3 and C4), with lowest C3 level on admission at 31 (Graph 1A). Decision was made to pursue eculizumab on 4/16/19 with continued clinical decline and no improvement in complement levels. She ultimately died on 4/24/19.
Patient 2 was a 35-year-old male with systemic lupus erythematosus (SLE), APS, end-stage renal disease, and Libman-Sacks endocarditis status post bioprosthetic aortic valve replacement admitted in February 2019 for worsening digital ischemia. Workup showed presence of lupus anticoagulant, thrombocytopenia, low C3 levels (Graph 1B), normal C4 levels, and arterial thrombi in the upper and lower extremities. Prior to initiation of treatment, respiratory status declined due to massive pulmonary embolus. He died after PEA arrest shortly thereafter.
Patient 3 is a 63-year-old male with chronic ITP and APS on warfarin, maintenance rituximab and intermittent apheresis admitted with worsening renal dysfunction in April 2019. Workup demonstrated acute on chronic thrombocytopenia, elevated APLA, and normal C3 and C4 levels (Graph 1C). Renal replacement therapy was commenced and he was discharged to receive ongoing outpatient therapy.
Patient 4 is a 35-year-old male with history of SLE and APS admitted in April 2019 with renal failure, anemia and thrombocytopenia. Workup showed presence of APLA. Despite therapy with steroids, IVIG, rituximab and TPEX he became anuric with renal biopsy showing thrombotic microangiopathy. He was also bacteremic with a mitral valve vegetation for which he underwent valve replacement. Hospital course was complicated by need respiratory failure necessitating intubation and ECMO. C3 levels were consistently low, but varied throughout his long admission (Graph 1D) and were not necessarily related to his clinical course (sepsis, ECMO, etc.). C4 levels were normal.
Conclusions:
Complement levels were variable among the patients in this case series. Three out of four patient had low C3, while only one patient had low C4. Further, complement levels did not improve in one patient after administration of eculizumab. Routine laboratory testing for C3 and C4 may not be optimal assays for monitoring disease status in CAPS. More specialized complement testing, such a C5 a/b, may be more appropriate especially in the setting of eculizumab use. While eculizumab is typically used in refractory disease, it may be pertinent to move this therapy into early line treatment to achieve better outcomes in certain clinical scenarios. Identification of a more specific biomarker to recognize cases in need of early therapy is warranted.
No relevant conflicts of interest to declare.
Eculizumab, a humanized monoclonal IgG antibody that binds to complement protein C5, is discussed for its off-label use in the treatment of catastrophic antiphospholipid antibody syndrome.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal