

Introduction:
Portal vein thrombosis (PVT) is usually associated with intra-abdominal malignancies, particularly pancreatic cancer (PC). PVT prevalence rate and impact on outcome of PC patients are not well studied, especially on a large scale of cohort. We described the prevalence and mortality trends of PVT amongst PC patients and analyzed their demographic characteristics. We also studied the impact of PVT with PC on hospitalization outcomes.
Methods:
We queried the 1998-2016 National Inpatient Sample (NIS) database of the Agency of Healthcare Research and Quality (AHRQ). Hospitalized adult patients (age≥18 years) with diagnosis of PC as well as presence of PVT were identified by using ICD-9 or ICD-10 codes. Cost of hospitalization was adjusted for inflation in reference to 2016. Comorbidities were classified using the Elixhauser comorbidity index. We used linear regression models to analyze trends in prevalence and outcomes over time. Logistic regression models were generated to evaluate multivariate predictors of length of stay (LOS), total charges, mortality, and complications in PC patients with and without PVT. The regression model was adjusted for age, sex, primary expected payer, teaching status of the hospital, hospital location, comorbid conditions, and presence of venous thromboembolism (VTE).
Results:
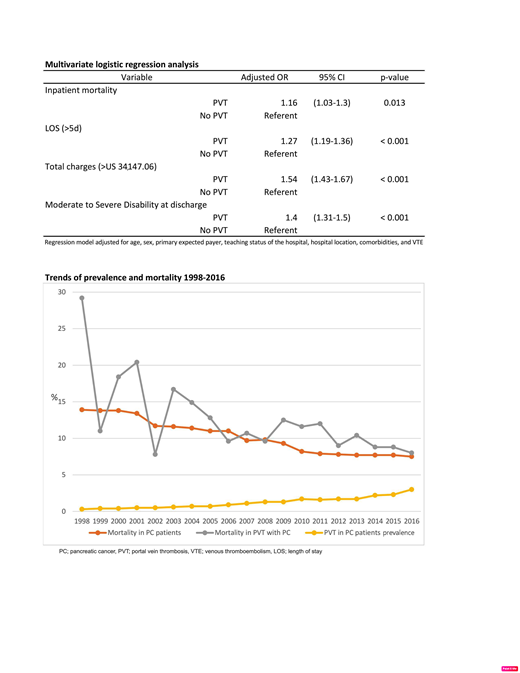
Among a total of 1,488,543 hospitalized PC patients, 19,725 (1.3%) experienced PVT. Mean age was 68 years. Hispanic Americans, younger age, teaching hospital, urban hospital and metastatic disease were associated with higher PVT prevalence rate. Interestingly, VTE prevalence in PC patients with and without PVT were 11% and 6% respectively, P<0.001. After adjusting for potential confounders, compared with those without PVT, PC patients with PVT had significantly higher inpatient mortality (10.5% vs 9.9%; odds ratio (OR), 1.16 [confidence interval (CI), 1.03-1.30]; P=0.013), longer LOS (8.29 vs 7.03 days; OR, 1.27 [CI, 1.19-1.36]; P<0.001), higher average cost of hospitalization (US $81,858 vs US $57,722; OR, 1.54 [CI, 1.43-1.67]; P<0.001), and greater likelihood of moderate to severe disability (defined as any beyond routine home discharge; ranging from short-term stay to skilled nursing facility to death upon discharge)(55.9% vs 51.3%, OR, 1.4 [CI, 1.31-1.50]; P<0.001). Although the annual prevalence of PVT among PC increased from 0.3% to 3.0% (p<0.001), in-hospital mortality declined significantly from 29.2% in 1998 to 8.0% in 2016 (p<0.001).
Conclusion:
In retrospective analysis of the NIS cohort of hospitalized patients with PC and PVT from 1998-2016, the prevalence increased by 10 folds. However, in-hospital mortality decreased significantly. Compared to those without PVT, patients with PC with PVT had higher inpatient mortality, longer length of stay, higher hospital cost and higher degree of disability upon discharge. Further studies are warranted to reveal a certain subgroup of PC patients who may benefit from prophylactic anticoagulation.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal