

Introduction
Pediatric acute Lymphoblastic Leukemia (ALL) patients have about 90% overall survival (OS) in developed countries. However, many children in low-middle income countries (LMIC) do not have access to appropriate drugs at optimal doses, a multidisciplinary medical team, laboratory resources for diagnosis and follow-up, and appropriate support therapy for morbidities and treatment-related toxicities. A 50-60% five-year OS has been reported in children with ALL in Mexico, and our center is not the exception. This low survival rate has pushed Mexican centers to develop strategies highlighting collaboration between centers with economic, research and teaching resources ("Mexico en Alianza con St. Jude MAS"), and outpatient treatment. However, each center must adapt their chemotherapy protocol to its own supplies and possibilities. We report the results of a risk adapted therapy protocol in a limited-resource treatment setting.
Materials and Methods
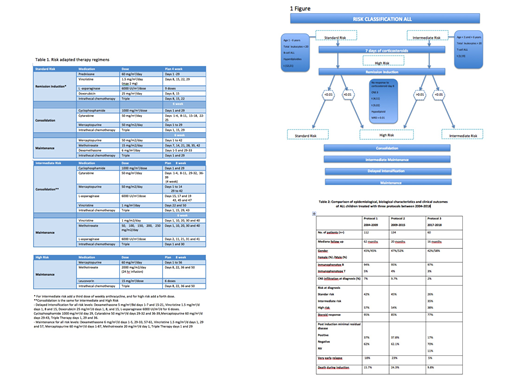
All pediatric patients with a diagnosis of ALL from January 2017 to December 2018 were classified according to risk as shown in Figure 1. Depending on risk classification, modifications to the induction, consolidation and intermediate maintenance regimens were made. The higher the risk, the higher the intensity of the regimen, as defined by the number of anthracycline doses, the presence or absence of high-dose methotrexate, and the duration of the consolidation and maintenance phases (Table 1). Demographic data is reported using distribution analysis, and the Kaplan-Meier method is used to analyze and predict overall survival, event-free survival (EFS) and relapse. Our results were compared with previous results from our institution.
Results
There were 35 male and 25 female patients; median age at diagnosis was 5.5. B-cell and T-cell lymphoblastic leukemia was the diagnosis in 57 (95%), and 3 (5%) patients, respectively, with a follow-up of 16 (8-30) months. Twenty-three (38%), 21 (35%), and 16 (26%) children were classified as high, intermediate and low risk ALL, respectively. After one week of corticosteroids 46 (77%) of patients had a good response. At the end of induction 53 patients had an evaluable MRD (88%), out of which 9 were positive (17%). Median follow-up was 16 (0.6-30) months. Mortality at induction was 6 (10%) patients. Very early relapse was observed in 3(5%) of patients. Estimated 2-year relapse rate was 6%, event-free survival was 84.1%, and OS was 85%. A comparison of results obtained with previous regimens (protocols 1 and 2) and the risk-adapted treatment (protocol 3) is observed in Table 2.
Conclusions
The implementation of a modified chemotherapy regimen based on adjusted stratification risk was associated to improved responses as reflected by MRD. A decrease in very early relapse rate to 5%, without increasing the toxicity and death during induction was observed.
Periodic and prospective outcome evaluation in a limited-resource setting is fundamental to adjust and to standardize therapy. Long-term follow-up of this patient group is required to compare OS and EFS at 5 years. This is a preliminary report, but it seems that we are changing the fate of Mexican children with ALL.
Gomez-Almaguer:Amgen: Consultancy, Speakers Bureau; Janssen: Consultancy, Speakers Bureau; Teva: Consultancy, Speakers Bureau; Takeda: Consultancy, Speakers Bureau; Celgene: Consultancy, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal