

Introduction:
Mixed phenotype acute leukemia (MPAL) is exceeding rare, making up less than 1% of all acute leukemias1, 2. It harbors features of both acute lymphoblastic leukemia (ALL) and acute myeloid leukemia (AML). Most cases have features of B-ALL; those with features of T-ALL are particularly uncommon2. We treated a 74-year-old retired male with T/myeloid MPAL. His disease progressed through 7 lines of therapy over 18 months, resulting in significant cytopenias and toxicity. Given the refractory nature of his disease to numerous ALL and AML-inspired regimens, we wanted to better understand trends in survival for this rare disease.
Methods:
The Surveillance, Epidemiology, and End-Result (SEER)-18 database was utilized, which encompasses 28% of the U.S. population. Patients of all ages diagnosed with T/myeloid MPAL between 2010-2016 were included. Patients with T-ALL and AML were used as comparators. The primary endpoint was disease-specific survival. Variables assessed included age, race/ethnicity, insurance type, geographical location, rural vs. urban location and socioeconomic status using county level data. Categorical variables were compared with the chi-square and fisher's exact test and survival was characterized with the cox proportional hazard model. This study was exempt from the IRB.
Results:
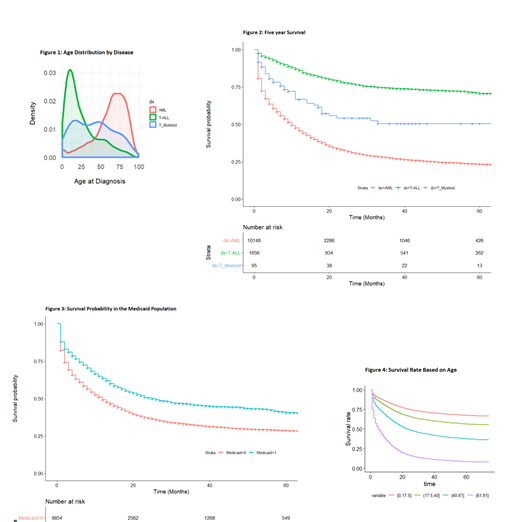
Ninety-five cases of T/myeloid MPAL were reported from 2010-2016 through the SEER-18 database. T/myeloid MPAL demonstrated a broad age distribution (median age: 40, IQR: 17-61), in comparison to T-ALL which mostly affected adolescence/young adults (median age: 17.5, IQR: 9-35) and AML which mostly affected older adults (median age: 67, IQR: 53-78) (figure 1). The 5-year survival was 50.4%, which was higher than AML (23.3%) and lower than T-ALL (70.6%) (figure 2). Survival did not change from 2010 to 2016. After adjusting for age, race/ethnicity, insurance type, geographical location, urban vs. rural location, and county level surrogates for poverty, the only two variables that significantly impacted survival were increasing age (HR 3.41, 95%CI: 2.13-5.46, p<.0001) and Medicaid insurance (HR 3.2, 95%CI: 1.27-8.09, p=.014) (figure 3-4). Estimated 5-year survival ranged from over 70% for children, adolescence and young adults to only 16% for older adults.
Discussion:
T/myeloid MPAL affects people of all ages. Given its rarity, there are no actively enrolling clinical trials or randomized controlled trials from which to guide management. Treatments are largely extrapolated from T-ALL and AML2. Despite newer FDA approved drugs for T-ALL and AML and improvements in allotransplant, survival has not improved and remains dismal for elderly patients. Older patients may have more aggressive disease biology and are often not candidates for intensive chemotherapy or allotransplant due to comorbidities and diminished reserve. Patient age very likely contributes to the difference in survival between T/myeloid MPAL and T-ALL or AML however Medicaid insurance also adversely affected survival in T/myeloid MPAL. This etiology is unclear, however could relate to decreased access to care.
Conclusion:
T/myeloid MPAL is an exceedingly rare disease with dismal outcomes in the elderly. A better understanding of the disease biology in elderly patients, insurance related barriers to care, and more personalized treatments are needed to improve patient outcomes.
References:
1. Mantutes E, Pickl WF, Van't Veer M, et al. Mixed-Phenotype acute leukemia: clinical and laboratory features and outcome in 100 patients defined according to the WHO 2008 classification: Blood 2001; 117:3163.
2. Wolach, O., & Stone, R. M. (2015). How I treat mixed-phenotype acute leukemia. Blood, 125(16), 2477-2485.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal