

Gemtuzumab Ozogamycin (GO) is a drug conjugated monoclonal antibody which targets CD33 an antigen highly expressed on the surface of AML blasts. GO is approved for the treatment of both newly-diagnosed and relapsed AML. Despite growing evidence regarding its efficacy and safety among AML patients there is limited data about the use of GO in isolated extra-medullary relapsed AML. Extramedullary AML remains as an unmet clinical need regarding the poor prognosis and lack of a standard therapeutic approach. Our cases demonstrated a rapid and long lasting response with a favorable toxicity profile, in patients who were treated with GO as a single agent after an isolated extramedullary relapsing disease.
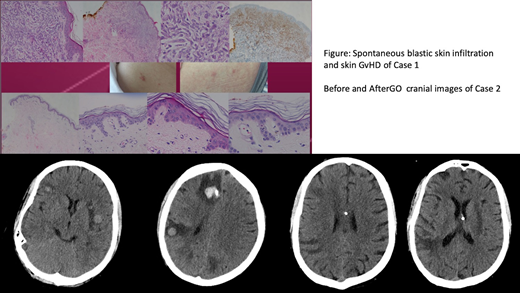
Our first case was a 40-years-old woman admitted to our outpatient clinic with pain in her joints and redness in her back and stomach. She was diagnosed with CD33-positive Acute Myeloid Leukemia according to the immunophenotyping of bone marrow blasts. Idarubicin and ARA-C (7+3) combination initiated as a frontline induction therapy and morphological remission was achieved after the first cycle of induction. After the first cycle of consolidation chemotherapy with high dose ARA-C she has relapsed with skin myeloid sarcomas and diffuse bone marrow infiltration. Soon after the relapsing disease she was put on to ida-flag salvage chemotherapy and she responded well with the disappearance of skin lesions and morphological complete remission of bone marrow. After achieving response, an allogeneic stem cell transplantation (HSCT) was applied from her sibling donor with a myeloablative conditioning. Unfortunately patient had a relapsing extramedullary disease with reappearance of skin lesions even with an ongoing acute skin gvhd (Figure) soon after allogeneic HSCT. Bone marrow biopsy revealed no increase in blast count.
We have decided to initiate a novel targetted therapy to control the extramedullary disease. As her blasts infiltrating the skin were universally CD 33 positive we considered to put her on GO therapy with the approval obtained from health authority. GO was applied according to the dosage approved by FDA for relapsing disease. After the first cycle of GO she had a rapid disappearance of all skin lesions just complicated with a febrile neutropenic episode and re-activation of CMV infection which was controlled with Gancyclovir. She has retained a complete remission regarding extramedullary disease throughout the repeated courses of GO for 3 times, and she is still in remission for 4 months after the first appearance of skin lesions (Figure).
Our second case was a 24-years-old boy who admitted to our outpatient clinic with a worsening fatigue and shortness of breath. He was also diagnosed with CD33-positive Acute Myeloid Leukemia according to the immunophenotyping of bone marrow blasts and was able to achieve a morphological CR after frontline induction therapy with 7+3 protocol. After two cycles of high dose ARA-C consolidation he was transplanted from a matched unrelated donor because of an intermediate cytogenetic risk profile. At the 14th month of allogeneic transplantation he had relapsed with a bone marrow blast count of 90% and harboring a monosomy on the 10th chromosome. After the first salvage chemotherapy with IDA-FLAG protocol he has achieved a morphological CR and we have decided to proceed with an alternative donor transplantation. But unfortunately soon after discharge, he has admitted to the emergency clinic with a new onset headache and nausea and vomiting. A cranial CT revealed multiple foci of solid masses with peripheral edema. We have performed a lumbar puncture and CSF fluid revealed a high number of CD33 positive blastic cells (over 100 cells per HPF). At the time of central nervous system (CNS) relapse his bone marrow was free of blastic infiltration. We decided to initiate GO treatment with the diagnosis of isolated central nervous system relapse of AML, accompanying intra-thecal chemotherapy via an Omaya Reservoir. He has received two cycles of GO which was complicated with neutropenic fever and grade 4 leukopenia and thrombocytopenia, and his CNS lesions also responded well and clinically he had no CNS related signs or symptoms. The patient received additional GO with continued response but unfortunately after a severe pneumonia he passed away at intensive care unit.
Our case series documented a clinically relevant therapeutic field for GO in isolated extramedullary relapse of AML.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal