

Introduction: Targeting immune cells in the tumor microenvironment is an attractive approach to improving antitumor activity of standard therapy in r/r hematologic malignancies. Durvalumab is a monoclonal antibody that blocks programmed cell death ligand-1 (PD-L1), allowing T cells to recognize and kill tumor cells.
Methods: The FUSION NHL-001 study (NCT02733042) is a phase 1/2 study assessing safety and efficacy of durvalumab as monotherapy or in combination. Eligible patients (pts) must have had r/r DLBCL or FL after ≥1 systemic therapy requiring therapeutic intervention. Other inclusion criteria include ECOG performance status 0-2 and ≥1 CT-measurable lesion. Pretreatment tumor biopsies were collected to assess biomarkers of response to durvalumab combination therapies.
Pts with r/r B-cell neoplasms were enrolled into 1 of 4 arms that included durvalumab monotherapy (Arm D) or in combination with lenalidomide ± rituximab (Arm A), ibrutinib (Arm B), or rituximab ± bendamustine (Arm C). Durvalumab was given at a fixed dose of 1500 mg every 4 weeks. The study consisted of 2 parts: dose finding (except for Arm D) to establish the recommended phase 2 dose (RP2D) for each combination and dose confirmation. We present final subset analyses for pts with DLBCL and FL treated in Arms A, C, and D.
Results: A total of 38 DLBCL and 22 FL pts were enrolled. Baseline characteristics are presented in Tables 1 and 2.
Arm A was prematurely closed after an FDA announcement regarding safety concerns with combination of lenalidomide and checkpoint inhibitors in multiple myeloma; therefore, RP2D for lenalidomide ± rituximab could not be defined. However, 4 pts (DLBCL, n=1; FL, n=3) experienced dose-limiting toxicities (DLTs): febrile neutropenia (lenalidomide 10 mg + rituximab), headache, hepatitis, and thrombocytopenia (lenalidomide 20 mg + rituximab).
One pt with DLBCL experienced DLT in Arm C (neutropenia) when treated with bendamustine 90 mg/m2 + rituximab. RP2D for bendamustine was established as 70 mg/m2.
Durvalumab treatment (13 infusions) was completed for 10 (DLBCL, n=4; FL, n=6) pts (17%), 2 in Arm A and 8 in Arm C; the main reason for durvalumab withdrawal was disease progression.
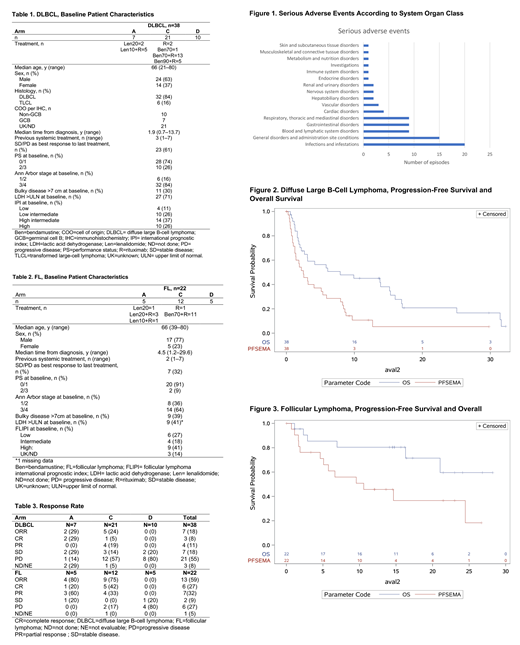
During the study, 38 pts (63%) experienced 81 serious adverse events (SAEs), most frequently related to infections (Figure 1). A total of 22 immune-mediated AEs (imAEs) related to durvalumab were reported in 13 pts (grade 1, 2, and 3 in 9, 7, and 6 cases, respectively): transaminitis and increased bilirubin (9 events), diarrhea (5 events), rash and pruritus (5 events), thyroid disorder (2 events), and infusion-related reaction (1 event). Two pts were treated with systemic steroids, both for grade 3 transaminitis. Others received symptomatic treatment. Ten pts experienced AEs that led to any drug discontinuation: 4 in Arm A (cerebral ischemia, febrile neutropenia, myalgia, hyponatremia), 3 in Arm C (transaminitis; neutropenia in 2 pts) and 3 in Arm D (drug reaction with eosinophilia and systemic symptoms, gastrointestinal perforation, prolonged QT). There were 6 grade 5 AEs, none considered related to study drugs.
For pts with DLBCL (Table 3), overall response rate (ORR) was 18% and complete response rate (CRR) was 8%. Median progression-free survival (PFS) (Figure 2) was 2.5 months (95% CI, 1.25-5.13). There were 30 deaths on study (2, 19, and 9 pts in Arms A, C, and D, respectively), 24 (80%) related to disease progression. Median overall survival (OS) was 7.9 months (2.66-15.31).
For pts with FL (Table 3), ORR was 59% and CRR was 27%. Median PFS (Figure 3) was 10.6 months (4.63-NE). There were 6 deaths on study (2 and 4 pts in Arms A and D, respectively); 3 (50%) were related to disease progression and 1 to second primary malignancy (bladder cancer, Arm A). Median OS was not reached.
An interferon-γ signature comprising 4 genes, IFN-γ, CD274, LAG3, and CXCL9, trended higher with best ORR in pts with r/r DLBCL (N=30, P=0.06) and FL (N=18, P=0.01) independent of treatment arm (Arms A, C, and D included in analysis).
Conclusions: Durvalumab as monotherapy or in combination in DLBCL and FL is tolerable without unexpected safety signals but requires close monitoring. Durvalumab alone or in combination appeared to add limited benefit to therapy for r/r DLBCL or FL. However, use of an interferon-γ gene signature may serve as a biomarker by which to enrich for r/r NHL pts that may be more responsive to anti-PD-L1-based therapy and will require further investigation.
Casulo:Gilead: Honoraria, Other: Travel, accommodation, expenses; Roche: Other: Travel, accommodation, expenses; Celgene: Research Funding. Santoro:MSD: Speakers Bureau; Lilly: Speakers Bureau; Sandoz: Speakers Bureau; BMS: Consultancy; Takeda: Speakers Bureau; BMS: Speakers Bureau; Abb-Vie: Speakers Bureau; Amgen: Speakers Bureau; Celgene: Speakers Bureau; AstraZeneca: Speakers Bureau; Pfizer: Consultancy, Speakers Bureau; Arqule: Consultancy, Speakers Bureau; Eisai: Consultancy, Speakers Bureau; Novartis: Speakers Bureau; Bayer: Consultancy, Speakers Bureau; Servier: Consultancy, Speakers Bureau; Roche: Speakers Bureau; Gilead: Consultancy, Speakers Bureau. Ando:Eisai: Research Funding. Le Gouill:Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel support; Roche-Genentech: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel support. Ruan:Celgene: Consultancy, Honoraria, Research Funding; AstraZeneca: Consultancy, Honoraria; Seattle Genetics: Consultancy, Honoraria, Research Funding; Janssen: Consultancy, Honoraria; Pharmacyclics LLC, an AbbVie company: Research Funding; Juno: Consultancy; Kite: Consultancy. Radford:Novartis: Consultancy, Honoraria; ADC Therapeutics: Consultancy, Research Funding; BMS: Consultancy, Honoraria; AstraZeneca: Equity Ownership, Research Funding; Seattle Genetics: Consultancy, Honoraria; Takeda: Consultancy, Honoraria, Research Funding; GSK: Equity Ownership. Arcaini:Celgene, Roche, Janssen-Cilag, Gilead: Other: Travel expenses; Gilead Sciences: Research Funding; Celgene: Speakers Bureau; Bayer, Celgene, Gilead Sciences, Roche, Sandoz, Janssen-Cilag, VERASTEM: Consultancy. Pinto:Roche: Speakers Bureau; Roche, Takeda: Other: Travel grants; EDO-Mundipharma: Patents & Royalties; Roche, MSD, Bristol-Myers Squibb, Servier: Honoraria; Servier, Roche, Bristol-Myers Squibb, MSD: Membership on an entity's Board of Directors or advisory committees. Izutsu:Eisai, Chugai, Zenyaku: Honoraria; Eisai, Symbio, Chugai, Zenyaku: Research Funding; Celgene: Consultancy; Chugai, Celgene, Daiichi Sankyo, Astra Zeneca, Eisai, Symbio, Ono, Bayer, Solasia, Zenyaku, Incyte, Novartis, Sanofi, HUYA Bioscience, MSD, Astellas Amgen, Abbvie, ARIAD, Takeda, Pfizer: Research Funding; Kyowa Kirin, Eisai, Takeda, MSD, Chugai, Nihon Medi-physics, Janssen, Ono, Abbvie, Dainihon Sumitomo, Bayer, Astra Zeneca, HUYA Japan, Novartis, Bristol-Byers Squibb, Mundi, Otsuka, Daiichi Sankyo, Astellas, Asahi Kasei: Honoraria. Rule:Astra-Zeneca: Consultancy, Honoraria; Gilead: Consultancy, Honoraria; Sunesis: Consultancy, Honoraria; Pharmacyclics: Consultancy, Honoraria; Celgene: Consultancy, Honoraria; Janssen: Consultancy, Honoraria, Research Funding; Roche: Consultancy, Honoraria, Research Funding; TG Therapeutics: Consultancy, Honoraria; Napp: Consultancy; Kite: Consultancy. Munoz:Pharmacyclics /Janssen: Consultancy, Research Funding, Speakers Bureau; Bayer: Consultancy, Speakers Bureau; Merck: Consultancy; Kyowa: Consultancy, Honoraria, Speakers Bureau; Seattle Genetics: Consultancy, Honoraria, Research Funding, Speakers Bureau; Celgene/Juno: Consultancy, Research Funding; Genentech: Consultancy, Research Funding, Speakers Bureau; Kite/Gilead: Consultancy, Research Funding, Speakers Bureau; Bristol-Myers Squibb: Consultancy; Alexion: Consultancy; Pfizer: Consultancy; Fosunkite: Speakers Bureau; AstraZeneca: Speakers Bureau; Portola: Research Funding; Incyte: Research Funding. Casadebaig:Celgene Corporation: Employment, Equity Ownership. Fox:Celgene Corporation: Employment, Equity Ownership. Rettby:Celgene Corporation: Employment, Equity Ownership. Dell'Aringa:Celgene Corporation: Employment, Equity Ownership. Delarue:Celgene Corporation: Employment, Equity Ownership. Newhall:Celgene Corporation: Employment, Equity Ownership. Czuczman:Celgene Corporation: Employment, Equity Ownership. Cartron:Roche, Celgene: Consultancy; Sanofi, Gilead, Janssen, Roche, Celgene: Honoraria.
Durvalumab is a PD-L1 blocking antibody indicated for the treatment of patients with 1) locally advanced or metastatic urothelial carcinoma who have disease progression during or following platinum-containing chemotherapy, or who have disease progression within 12 months of neoadjuvant or adjuvant treatment with platinum-containing chemotherapy, or 2) unresectable, stage 3 NSCLC whose disease has not progressed following concurrent platinum-based chemotherapy and radiation therapy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal