

Background: Chronic lymphocytic leukemia (CLL) has a classic immunophenotype, consisting of light chain restriction, CD5+, CD19+, dim CD20, CD23+, CD43+, CD200+, CD10- and CD79b-. This distinguishes it from normal B cells and other lymphoproliferative disorders (LPDs). Antibodies targeting these antigens are included in two 8-color flow cytometry panels developed by the Euroflow consortium for the work up of B cell LPDs. Combining these antibodies into one 10-color panel would be more cost-effective. Furthermore, new CLL therapies can induce deep remissions, creating an increasing demand to measure minimal residual disease (MRD), defined as having over 1 residual leukemic cell per 10,000 leukocytes (10-4). The current international standardized approach for measuring MRD established by the European Research Initiative on CLL (ERIC) uses a panel of antibodies targeting CD3, CD5, CD19, CD20, CD22, CD43, CD79b and CD81. However, these antibody-fluorochrome combinations are different than those used by the Euroflow diagnostic panels. Thus laboratories considering implementing MRD testing would need to purchase antibodies for 3 different panels (2 diagnostic and 1 MRD). We expanded the Euroflow 8-color lymphocyte screening tube (LST) to include CD200 and CD23, such that CLL can be detected in one 10-color tube, at levels as low as 0.01%. The goal of this study was to determine the potential cost savings in implementing this new panel and to determine if it is sensitive enough to detect MRD.
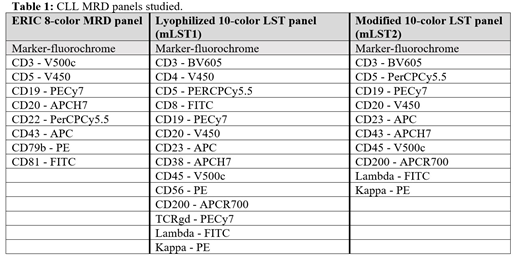
Methods: We calculated the number of samples analyzed with our modified 10-color LST tube (mLST1, obtained lyophilized) from April 2018 to March 2019 to rule out an LPD and the number of antibody aliquots saved using this approach compared to the standard 2-tube Euroflow method. We also created a version of the above-mentioned panel (mLST2) using liquid antibodies to increase the generalizability of our results, substituting CD38 with CD43 to see if this improved MRD detection (see panels below). For MRD testing, we used CLL samples from 24 different patients to produce 60 MRD samples at various concentrations of leukemic cells. Samples were prepared by spiking CLL cells into suspensions of normal leukocytes at approximate concentrations of 0.1%, 0.01% and 0.001%. Each sample was aliquoted and stained with the three panels: ERIC, mLST1 and mLST2. Data was acquired using a BD FACSCanto II or a BD FACSAria Fusion and analysed using BD FACSDiva software. CLL cells were identified based on differential expression of key markers and MRD was calculated as the number of CLL cells/total leukocytes. MRD positivity was defined as ≥ 0.01%. Agreement between the panels was assessed using the Bland-Altman plot method. We also calculated the percentage agreement between the panels in identifying MRD positivity.
Results: In 1 year, mLST1 was performed on 474 samples, of these 220 had an LPD and 123 (56%) had a classic CLL phenotype, obviating the need for further testing. This resulted in the net savings of 476 antibody aliquots. For MRD assessment, differential expression of CD5 and CD20 were the most significant contributors in distinguishing CLL from normal B cells using the mLST1 and mLST2. We identified one CLL case with an atypical immunophenotype (dim CD5, bright CD20) which proved difficult to gate using a mLST panel. There was agreement in MRD results obtained with the mLST panels and the ERIC panel. For values above the limit of quantification, the 95% limit of agreement was ±0.3369 log for the ERIC vs mLST1 comparison and ±0.3485 log for the ERIC vs mLST2 comparison. Thus, variability in MRD levels between the panels was less than 2-fold the majority of the time, which we considered clinically acceptable as MRD is measured on an exponential scale. The ERIC panel and the mLST1 had 88.3% agreement in distinguishing MRD-positive versus MRD-negative samples. Agreement was 93.3% between the ERIC panel and the mLST2.
Conclusions: Using a modified 10-color LST panel for both diagnosis and MRD measurement of CLL is feasible. The advantages are increased familiarity with the antibodies and potential cost savings, making MRD accessible to more cytometry laboratories. Atypical CLL cases without the usual CD5 positivity and dim CD20 are very difficult to gate using an LST panel. In these cases, the ERIC panel is clearly superior as CD22, CD79b, CD81 and CD43 can still provide separation between the malignant and normal lymphocytes.
Bazinet:BD Biosciences: Other: Provided a significant amount of the antibodies used in this project free of cost.. Wever:Teva Canada Innovation: Employment. Gimmig:BD Biosciences: Employment. Johnson:Lundbeck: Employment, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel fees, gifts, and others, Research Funding; Merck: Consultancy, Honoraria; Roche: Consultancy, Employment, Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: Travel fees, gifts, and others, Research Funding; Abbvie: Consultancy, Employment, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; BD Biosciences: Other: Provided a significant proportion of the antibodies used in this project free of cost.; BMS: Consultancy, Honoraria; Seattle Genetics: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal