

Background: Diffusion-weighted whole body MRI (WB-DWI) is a new functional imaging technique comprising anatomical and functional sequences with an emerging role in the management of multiple myeloma (MM) patients (pts) since it allows highly sensitive detection of diffuse bone marrow (BM) infiltration pattern and focal lesions, avoiding intravenous injections and radiation exposure. The aims of our study were 1) to test the correlation between plasma cells infiltration (BMPC) rate at BM biopsy and the presence of diffuse infiltration pattern at WB-DWI. 2) to compare response according to IMWG criteria and WB-DWI response and to establish the rate of discordancy (WB-DWI progression with increased focal lesions and at least a partial response according to IMWG criteria)
Methods: We reviewed data regarding 45 MM patients (pts) observed in our Centre between September 2018 and July 2019 for whom quantification of serum and urine monoclonal component (MC), free light chains value (FLC), BM biopsy, whole body CT scan and WB-DWI data were available at the same time point. Sequential assessment of WB-DWI and laboratory data was available in 20 pts. Patients performed a WB-DWI (Magnetom Area, 1.5T, Siemens Enlarged Germany) for head to knee. The protocol included anatomical sequences T1 and T2 weighted with fat suppression on the sagittal plane specifically for the spine. Coronal T2 weighted fat suppression sequences are performed for the study of femural bone. Axial Dixon T1 weighted sequences of the whole scan region, in breath-old. The functional part is formed by diffusion weighted sequences in the axial plane. MM diagnosis and response were assessed by IMWG criteria. Response were categorized as follows: responsive patients if ≥PR, progressive disease if <PR. BM infiltration rate was used as a continuous variable. WB-DWI findings at first evaluation were categorized as follows: presence/absence of focal lesions, presence/absence of diffuse pattern of BM infiltration. Radiological re-assessment of both focal lesions and diffuse pattern was categorized as follows: reduced/stable/increased. Discordant pattern of progression was defined as: ≥PR + diffuse pattern stable/reduced + focal lesions increased. Association between two categorical variables was evaluated by Fisher's exact test. Mann-Whitney test was used to compare a quantitative variable among two independent groups of patients. P-values<0.05 were considered significant.
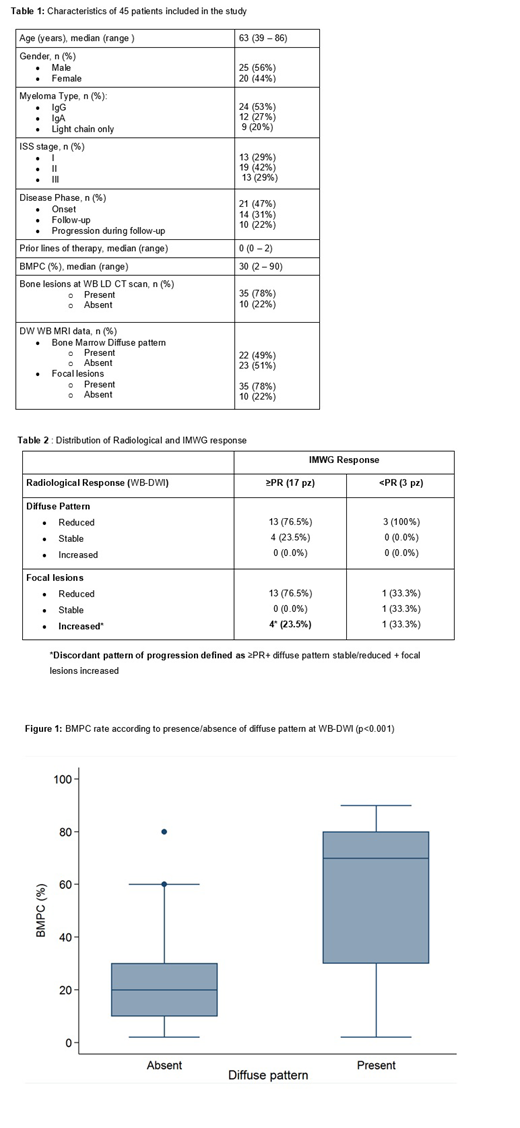
Results: Table 1 summarizes the clinical and radiological data of the population on study. Median age was 64 years (range 38-86), median number of previous lines of therapy at time of evaluation was 0 (range 0-)2; 47% pts were at the onset, 31% were in follow-up after treatment completion, 22% had progressive disease.
WB-DWI showed a diffuse pattern in 22 pts (49%); in 23 patients without a diffuse pattern, 7 (30%) had PBMC >10%; BMPC infiltration rate was significantly higher in pts with presence of diffuse pattern at WB-DWI (p<0.001; Figure 1). WB-DWI showed focal lesions in 35 pts (78%): 19 of them were at onset of disease. Most of the patients performing sequential assessment of WB-DWI were responsive according to IMWG criteria at time of WB-DWI re-evaluation (17 pts with ≥PR, 85%). Table 2 shows radiological findings according to IMWG response. Focusing on patients with ≥PR, WB-DWI diffuse pattern was reduced in 13 pts (76.5%) and stable in 4 pts (23.5%) with complete concordance between hematological and radiological findings (increased diffuse pattern in no pt with ≥PR); focal lesions were reduced in 76.5% and increased in 23.5%; a discordant pattern of progression was found in 4 patients (20%).
Conclusions: Our study findsa significant correlation between presence of WB-DWI diffuse infiltration patter and BMPC rate, highlighting the possible future use of this radiological technique for monitoring BM residual disease. In addition, this study shows the possible not negligible emergence of discordant pattern of progression, probably deriving from the spatial heterogeneity of MM clones and their different sensitivity to therapy.
Mangiacavalli:celgene: Consultancy; Janssen cilag: Consultancy; Amgen: Consultancy. Varettoni:Gilead: Other: travel expenses; ABBVIE: Other: travel expenses; Roche: Consultancy; Janssen: Consultancy. Arcaini:Celgene: Speakers Bureau; Celgene, Roche, Janssen-Cilag, Gilead: Other: Travel expenses; Gilead Sciences: Research Funding; Bayer, Celgene, Gilead Sciences, Roche, Sandoz, Janssen-Cilag, VERASTEM: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal