

Background
Secondary malignancies (SM) are a recognized complication following allogeneic hematopoietic stem cell transplant (HCT). It is unclear whether specific immunosuppressive therapies (IST) may contribute to this risk. We have reported that Azathioprine (AZP) is a relevant option as a steroid-sparing agent in chronic graft versus host disease (cGvHD) treatment (Uhm et al BMT 2018) by evaluating its failure-free survival and overall survival.
AZP is known to increase the risk of SM in patients with inflammatory bowel disease or autoimmune disease. Also, cGvHD in of itself increases the risk of SM. However, SM risk was not extensively investigated in patients treated with AZP for cGvHD. Thus, we performed a retrospective chart review to evaluate IST and analyze for correlations with SM risk and whether treatment with distinct IST, including AZP, may be associated with added risk for SM development.
Patients and methods
A total of 502 patients who received HCT from Jan 2000 to Dec 2012 and had a diagnosis of cGvHD according to NIH criteria after HCT, treated from April 2000 to Mar 2013, at Princess Margaret Cancer Center, Canada, were enrolled in the retrospective study. Patients and disease characteristics are as follows: median age of 48 years; male 289 (57.6%), classical 217 (43.6%), overlap syndrome 281 (56.4%). Of note, 394 patients (78.6%) had a previous history of acute GvHD. Subtype, severity and organ involvement of cGvHD were assessed at initial presentation of cGvHD. The most common treatment used for cGvHD was systemic corticosteroid (82.7%) followed by AZP (40.8%), cyclosporine (CSA) (40.1%) and mycophenolate mofetil (MMF) (26.5%).
The incidence of SM was calculated from HCT to the first day of confirmed diagnosis of SM using cumulative incidence method considering competing events such as relapse or death. Risk factors for SM development were compared using Gray model. Survival after diagnosis of SM was calculated using Kaplan-Meier estimates and compared using log-rank test. For multivariate analysis, Fine-Gray regression model and Cox proportional hazard model were used to analyze the effects of variables on SM risk and survival (OS), respectively.
Results
With a median follow-up duration of 12.3 years, 101 patients were diagnosed with SM with a median onset of 5.7 years (range 0.3-18.3 years). The most common types of SM were basal cell skin cancer (n=29), followed by squamous cell skin cancer (n=22) and head & neck cancer (n=17). The overall incidence of SM was 19.5% (95% CI, 15.9-23.4%) at 12 years.
We evaluated multiple risk factors for the risk of SM, and the following variables were not statistically significant: the use of fludarabine, total body irradiation, stem cell source, donor type, previous acute GvHD, use of T-cell depletion, subtype and severity of cGvHD, organ involvement of mouth, eye, liver, gut, lung, musculoskeletal system at initial presentation. In addition, we evaluated the use of systemic IST including corticosteroid, CSA, tacrolimus, MMF and ECP but with no effect on SM risk.
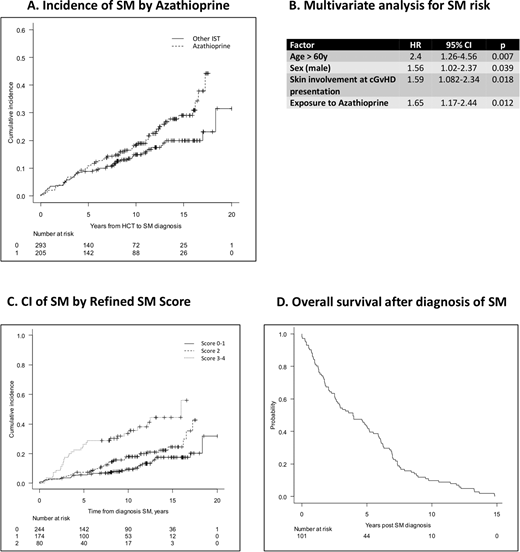
Of interest, the use of AZP was found to increase the risk of SM: The cumulative incidence of SM was 22.7% (16.9-29.1%) at 12 years in the AZP group, whereas it was 16.9% (12.5-21.9%) in those treated without AZP (p=0.023) (Fig A). Exposure duration of AZP showed good correlation with increased risk of SM: patients treated with AZP for 5.85 years or longer showed 46% higher risk of SM development than those not (HR 1.46 [1.11-1.91], p=0.007).
Multivariate analysis confirmed the following factors as risk factor for SM: exposure to AZP (HR 1.65, p=0.012), age at transplant >60 years (HR 2.40, p=0.007), male sex (HR 1.56, p=0.039) and skin involvement at cGvHD presentation (HR 1.59, p=0.018) (Fig B).
A refined SM risk score was developed, giving a point each for age over 60 years, male sex, skin involvement at cGvHD presentation, and exposure to AZP. The summed scores were grouped 0-1 (n=244), low risk of 13.3%; 2 (n=174), intermediate risk of 19.9% (HR 1.614); above 2 (n=80), high risk for SM, 38.1% at 12 years (HR 3.502; p<0.001) (Fig C).
Median survival duration was 3.9 years after SM diagnosis, while 5 year survival rate was 43.6% (33.8-52.9%) (Fig D). The use of AZP does not appear to affect survival after diagnosis of SM.
Conclusions
The present study suggests that the use of AZP correlates with the risk of SM after adjustment of other confounding covariates such as skin involvement of GVHD, patient age or sex.
Lipton:Takeda: Consultancy, Honoraria, Research Funding; Novartis: Consultancy, Research Funding; Pfizer: Consultancy, Honoraria, Research Funding; BMS: Consultancy, Research Funding; Ariad: Consultancy, Research Funding; Bristol-Myers Squibb: Honoraria. Mattsson:Jazz Pharmaceuticals: Honoraria; ITB: Honoraria; Gilead: Honoraria; Mallinkrodt: Honoraria; Takeda: Membership on an entity's Board of Directors or advisory committees.
Azathioprine is being used to treat chronic gvhd

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal