

Introduction: Genetic risk factors play an important role in the prognosis of a patient with Chronic Lymphocytic Leukemia (CLL) or Small Lymphocytic Lymphoma (SLL). One of the strongest negative prognostic factors is the presence of a 17p deletion (del(17p)). While ibrutinib monotherapy has shown efficacy in the relapsed/refractory and treatment-naïve settings (Burger et al., 2015; Munir et al., 2019), evidence from clinical trials specifically concerning its use in patients with del(17p) is limited in the front line setting. The available limited evidence does suggest that its use in patients with del(17p) may result in shorter PFS and OS compared to patients without the deletion (Mato et al., 2018; O'Brien et al., 2018; Brown et al., 2018). Using real world data we addressed two objectives: (1) comparing baseline demographic and clinical characteristics of ibrutinib-treated patients with and without del(17p), and (2) assessing outcomes of overall survival (OS), time-to-next-treatment (TTNT), and time-to-treatment discontinuation (TTD) among CLL/SLL patients with and without del(17p) in the first-line setting.
Methods: Data from the nationwide Flatiron Health EHR-derived de-identified database were abstracted. Patients included were those aged ≥18 years, diagnosed with CLL/SLL (ICD-9 codes: 204.1x or ICD-10: C91.1x, C83.0x), and who had at least two clinic encounters in the Flatiron Health network and received ibrutinib as first CLL directed therapy on or after January 1, 2011. Patients had documented CLL/SLL and a documented cytogenetic test performed prior to ibrutinib start date confirming the presence or absence of del(17p). The start of first-line ibrutinib was defined as the index date for all comparative analyses. Baseline characteristics between present or absent del(17p) groups were compared. OS, TTNT, TTD were estimated using Kaplan Meier method and survival outcomes were compared between the two groups using the Cox proportional hazards model. Adjustment for covariates was performed for gender, age at index date, practice type (academic or community), Rai stage at diagnosis, ECOG status year of index date, status of deletion 11q, 13q, Trisomy 12 and IgHV mutation status. Reasons for discontinuation of ibrutinib are being explored. Presence or absence of TP53 mutations were not captured.
Results: There were 1,037 first-line ibrutinib treated patients included based on the above inclusion criteria, 24% of patients had del(17p) present. The majority (95%) of patients were treated in community practices and the median follow up period was 18 months.
The two groups differed in their Rai stage distribution at diagnosis, with del(17p) present patients tending to be later stage at diagnosis than del(17p) absent. Del(17p) patients also started first-line therapy sooner after diagnosis.
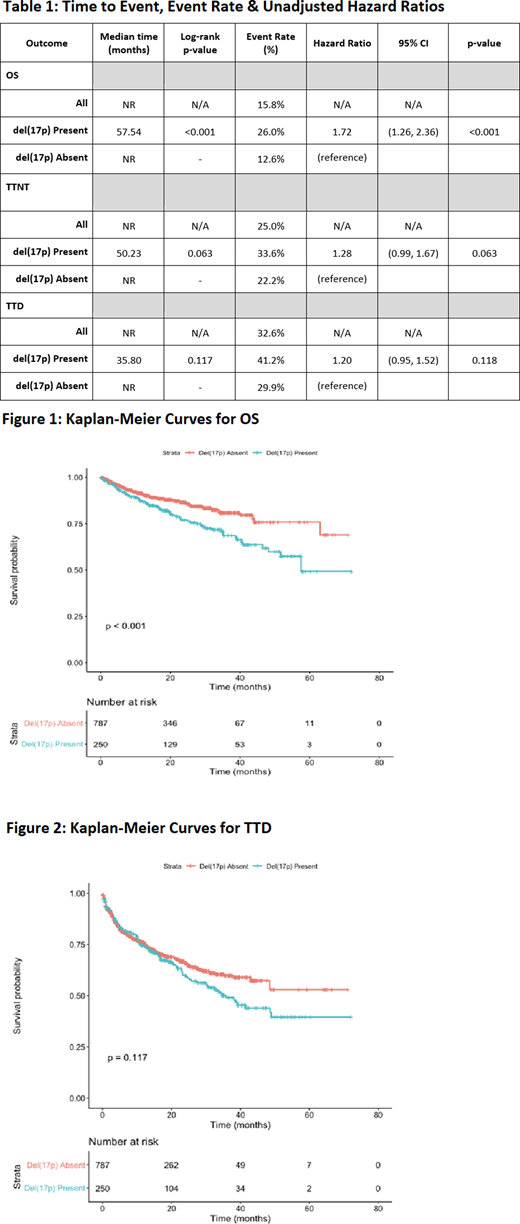
Median OS was shorter in the del(17p) present group at 57.54 months from initiation of treatment (p<0.001), compared to the del(17p) absent group where median OS was not reached [Table 1, Figure 1].
The Cox proportional hazards models were consistent with this finding, where HR for OS was 1.72 times greater in the del(17p) present group, and this difference was statistically significant in both the unadjusted (p<0.001) [Table 1] and adjusted analyses (p=0.009) [Not shown].
In parallel with OS findings, the del(17p) present group tended to have shorter median TTNT (50.23 months vs. NR, p=0.063). The TTD for all patients was 48.62 months, while the TTD was shorter in the del(17p) group (35.80 months vs. NR, p=0.117). These results were confirmed in the Cox proportional hazards models and similarly the difference between groups was not statistically significant [Table 1, Figure 2].
Conclusions: We present the largest study addressing outcomes of patients with del(17p) treated with ibrutinib monotherapy in the front line setting to address an important data gap that current clinical trials have not directly addressed. Since ibrutinib is now a standard of care for such high-risk patients, a deeper understanding if the presence of del(17p) impacts survival outcomes in patients treated with ibrutinib in the front line setting is needed. Based on the significant impact shown on OS, and to a lesser degree TTNT and TTD, these data confirm that del(17p) is a negative predictive factor in this setting. This reflects an ongoing unmet need among treatment naïve CLL/SLL patients with del(17p) status.
Mato:Janssen: Consultancy, Research Funding; Loxo: Consultancy, Research Funding; Genentech: Consultancy, Research Funding; Pharmacyclics: Consultancy, Research Funding; TG Therapeutics: Consultancy, Research Funding; AstraZeneca: Consultancy, Research Funding; AbbVie: Consultancy, Research Funding; Adaptive: Consultancy, Research Funding. Tang:BeiGene, Ltd.: Current Employment, Current equity holder in publicly-traded company. Azmi:BeiGene, Ltd.: Current Employment, Current equity holder in publicly-traded company. Yang:BeiGene, Ltd.: Current Employment, Current equity holder in publicly-traded company. Stern:BeiGene, Ltd.: Current Employment, Current equity holder in publicly-traded company. Hedrick:BeiGene, Ltd: Current Employment, Current equity holder in publicly-traded company. Huang:BeiGene: Current Employment, Current equity holder in publicly-traded company, Other: TRAVEL, ACCOMMODATIONS, EXPENSES (paid by any for-profit health care company). Sharman:AbbVie: Consultancy, Research Funding; Bristol Meyers Squibb: Consultancy, Research Funding; BeiGene: Research Funding; Pfizer: Consultancy, Research Funding; Pharmacyclics: Consultancy, Research Funding; AstraZeneca: Consultancy, Research Funding; Genentech: Consultancy, Research Funding; TG Therapeutics: Consultancy, Research Funding; Acerta: Consultancy, Research Funding; Roche: Consultancy, Research Funding; Celgene: Consultancy, Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal