

Background: Patients (pts) with hematologic malignancies (HM) are thought to have suboptimal hospice utilization and receive more aggressive end of life (EOL) care than those with solid tumors (ST), including high rates of EOL chemotherapy use, ICU admissions, and inpatient deaths (Egan, Blood Adv, 2020). Barriers to equitable EOL care outcomes for pts with HM may include difficulty identifying the "terminal phase" of disease, the potential for curative stem cell transplant that lingers even after failure of multiple therapies (Odejide, JCO, 2016), and specificity of palliative needs in HM, like transfusion dependence (Leblanc, Blood, 2018), that are not met by the current hospice benefit. However, direct comparison of EOL outcomes between HM and ST in a population-based setting has not been conducted. Our objective was to compare EOL care quality measures, hospice utilization, and indicators of palliative needs between Medicare beneficiaries with HM and ST.
Methods: From the linked SEER Medicare database (covering ~30% of the US population), we identified beneficiaries with common ST (breast, prostate, lung, and colorectal cancer) and HM (leukemia, myeloma, lymphoma, myelodysplastic syndrome [MDS], and myeloproliferative neoplasms [MPN]) who died between 2011-2015, and whose cause of death was cancer. We ascertained claims-based indicators of EOL care quality: hospice use before death, duration of hospice length of stay (LOS), death in an acute care hospital, receipt of (oral or parenteral) chemotherapy in the last 14 days of life (DOL), ICU admission in the last 30 DOL, Medicare spending, and inpatient days in the last 30 DOL. We also explored indicators of palliative needs: opioid use, transfusion use, and number of physician office visits in the last 30 DOL. We compared binary outcomes in multivariable robust Poisson (reporting adjusted relative risk, adj RR), counts in negative binomial, and costs in log-gamma models, reporting estimates with 95% confidence intervals (CI). Models were adjusted for age, sex, race, marital status, Medicaid co-insurance (indicator of low socio-economic status), prevalent poverty, comorbidity index, performance status indicator, calendar year, and survival from diagnosis.
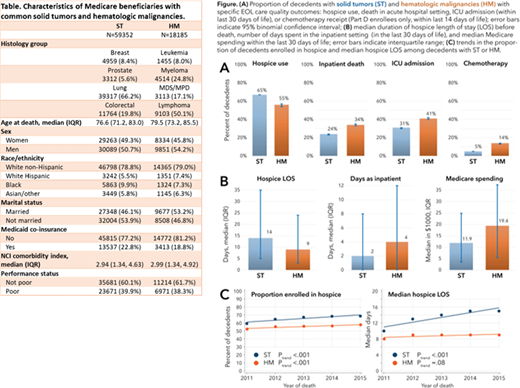
Results: Characteristics of the 18,185 patients with HM and 59,352 with ST are listed in Table. HM pts were, on average, older, and more likely to be male and married. HM pts were less likely than ST pts to enroll on hospice (58% vs 67%, adjusted RR 0.85,CI 0.84-0.86), had a shorter hospice LOS (median 9 vs 14 days, adj means ratio RR 0.81, CI 0.79-0.83), and were more likely to spend < 3 days on hospice (adj RR 1.29, CI 1.24-1.35) (see Figure). HM pts were more likely to die in an acute care setting (32% vs 23%, adj RR 1.4, CI 1.36-1.44), have an ICU admission in the last 30 DOL (39% vs 30%, adj RR 1.32, CI 1.29-1.35), and receive chemotherapy in the last 14 DOL (12% vs 5%, adj RR 2.73, CI 2.55-2.93). Median Medicare spending in the last 30 DOL was higher in HM than in ST (17.8k vs 11.9k, adj means ratio 1.52, CI 1.49-1.56), as was the median number of inpatient days (4 vs 2, adj means ratio 1.55, CI 1.52-1.59). The results were consistent when examined by specific subtypes of HM and ST. Pts with HM were less likely to use opioids at the EOL (adj RR 0.81, 95% CI, 0.79-0.84), but had more transfusions (adj RR 4.34, 95% CI, 4.11-4.58) and more physician office visits (adj RR 1.11, 95% CI, 1.09-1.14). Furthermore, trends in EOL care quality indicators differed between HM and ST. While the use of hospice services increased for both populations, the hospice LOS has steadily lengthened over time in ST (from median 10 days in 2011 to 14 days in 2015, P<.001), but it did not change significantly in HM (P=.077).
Discussion: To our knowledge, this is the first population-based study demonstrating that, adjusting for socio-demographic characteristics and baseline health status, pts with HM have inferior EOL care quality outcomes than those with ST. These disparities are consistent across all established EOL care quality outcomes and across all histologies, supporting the notion of a fundamental difference between EOL care in HM and ST. Furthermore, our data challenge the assumption that HM pts do not have significant palliative care needs; rather, their needs may differ from those of ST patients, and may be less easily met by the current hospice benefit (as other literature suggests). Novel care models are needed to improve EOL care for pts with HM.
Panagiotou:International Consulting Associates, Inc: Other: personal fees from International Consulting Associates, Inc. outside the scope of the submitted work. LeBlanc:AstraZeneca: Research Funding; Agios, AbbVie, and Bristol Myers Squibb/Celgene: Speakers Bureau; UpToDate: Patents & Royalties; American Cancer Society, BMS, Duke University, NINR/NIH, Jazz Pharmaceuticals, Seattle Genetics: Research Funding; AbbVie, Agios, Amgen, AstraZeneca, CareVive, BMS/Celgene, Daiichi-Sankyo, Flatiron, Helsinn, Heron, Otsuka, Medtronic, Pfizer, Seattle Genetics, Welvie: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees. Olszewski:Adaptive Biotechnologies: Research Funding; Spectrum Pharmaceuticals: Research Funding; Genentech, Inc.: Research Funding; TG Therapeutics: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal