

Sickle cell disease (SCD) is a severe hemoglobinopathy due to the production of abnormal hemoglobin S (HbS). Although red blood cell (RBC) dysfunction is the major contributor to disease, several studies highlighted the important role of polymorphonuclear neutrophils (PMNs), both during acute and chronic complications. One of the most severe complication of SCD is ischemic stroke due to large cerebral artery occlusion. In 1998, the Stroke Prevention (STOP) trial demonstrated that monthly blood transfusions could reduce the risk of stroke by 90% in SCD children with cerebral vasculopathy (CV). However, there is a wide heterogeneity in the course of CV in patients receiving chronic transfusions, since only about half of them improved their CV under transfusion program, while 25% are only stabilized and 29% continue to get worse despite a percentage of HbS permanently below 30%.
The aim of our study is to investigate the impact of transfusion programs on neutrophils activation and ageing, in order to identify if inflammation could contribute to the persistence of SCD complications despite red cell transfusion.
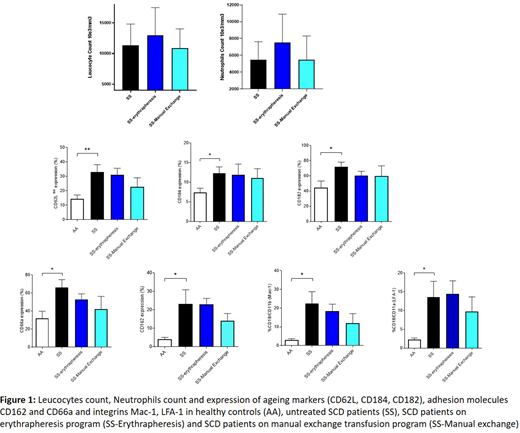
We performed a prospective study including 58 homozygous SCD children and 10 healthy donors. Of these, 12 had no specific treatment, 11 were on Hydroxyurea (HU) treatment, 21 were on an exchange transfusion program, and 14 were on both an exchange transfusion program and HU treatment for an average of 4.9 years due to persistent CV. Monthly exchange transfusion are carried out either by erythrapheresis or by manual exchanges, consisting of the continuous bleeding of whole blood compensated by simultaneous transfusion of packed red blood cells. Neutrophils were isolated from fresh blood samples before exchange transfusion session and labelled with 8 markers specific of adhesion, activation and ageing. We quantified by flow cytometry the expression of 3 integrins (CD18, CD11a, CD11b), 3 ageing markers (CD182, CD184, CD62L) and 2 adhesion molecules (CD162 and CD66a). We also measured the plasmatic level of elastase, which reflects the NETose activity of PMNs
As previously reported, we observed a high leukocytosis and an activated profile of PMNs in the 12 non-transfused SCD patients compared to healthy controls (Figure 1), characterized by an overexpression of the integrin CD18/CD11b (p=0,03) and CD18/CD11a (p=0,02), a higher level of circulating aged PMNs CD184 high/CD62Llow (p=0,04), a higher expression of CD162 (p=0,01) and CD66a (0,01) as well as a higher plasmatic level of elastase (p=0.01).
Interestingly, in the PMNs of the 21 patients receiving monthly exchange transfusion, we found an identical expression pattern of integrins, selectins, ageing markers and elastase level compared to those of the PMNs from non-transfused patients. Furthermore, we also observed a persistence of high neutrophilic leukocytosis. This activation pattern was the same for patients on manual exchange or erythrapheresis, even with a tendency towards a more inflammatory profile in patients on erythrapheresis (Figure 1).
In the PMNs from the 11 patients receiving HU compared to untreated SCD patients, we found an expected decrease in high leukocytosis and membrane integrin expression CD18/CD11b and CD18/CD11a. The addition of HU therapy in 14 patients in exchange transfusion program allows to alleviate neutrophilic leukocytosis and membrane integrin expression.
Our study shows for the first time that replacing sickle RBCs with healthy RBCs is not sufficient to reverse the pathological phenotype of PMNs in SCD. A persistence of the PMNs activation pattern is observed both despite erythrapheresis, where plasma and white blood cells go back to the patient, and in manual exchanges, where the patient is bled from a large volume of whole blood. Given the major role of inflammation in endothelial damage and vasculopathy in SCD, our data could explain the incomplete efficacy of transfusion exchange programs to treat CV. This raises the question to systematically combine anti-inflammatory and anti-white blood cell adhesion treatments such as Hydroxyurea or P-Selectin inhibitors for these patients.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal