

Background
Treatments for 'accelerated phase' MPNs (MPN-AP, 10-19% blasts)/post-MPN AML (MPN-BP, ≥20% blasts) are limited. Most patients are precluded from potentially curative haematopoietic stem cell transplantation (HSCT). For HSCT ineligible patients, azacitidine (AZA) is licensed to treat high-risk MDS or AML. Whilst dose and toxicity profile of AZA is well understood, the response of MPNs and post-MPN AML to monotherapy is limited. AZA-based doublet chemotherapy may however result in improved clinical responses. The phase Ib single-arm PHAZAR trial was established to determine maximum tolerated dose (MTD), safety profile and clinical activity of the selective JAK1/2 inhibitor ruxolitinib (RUX) used in combination with AZA to treat MPN-AP and MPN-BP patients.
Methods
A modified two-stage continual reassessment method with an expansion cohort at the MTD, was used to establish the MTD of RUX in combination with AZA. Successive flexible cohorts of 3-5 patients were enrolled at a fixed AZA dose of 75 mg/m2 s/c for 7 days (excluding weekends, on a 5-2-2 schedule) of a 28-day cycle with continuous administration of an allocated oral RUX dose (dose levels 0, 1, 2 and 3 = 10, 15, 20 and 25 mg BD respectively), and a formal response assessment recorded after 6 cycles. Toxicities were prospectively recorded as per CTCAE v4.0 with dose limiting toxicity (DLT) defined as a grade 3 or 4 non-haematological toxicity during treatment cycle 1. Clinical activity was evaluated over 12 months through assessment of bone marrow response after 3 and 6 treatment cycles, progression free survival (PFS), leukaemia free survival (LFS) and overall survival (OS).
Results
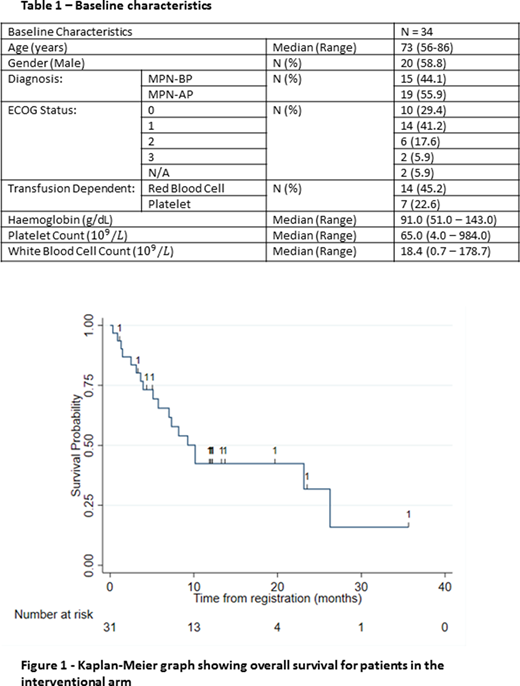
Thirty four advanced phase MPN patients were recruited from 12 Trials Acceleration Programme sites (19 MPN-AP; 15 MPN-BP). Baseline characteristics are summarized in Table 1. Driver mutation status was available for 25/34(74%) patients. 17/25(68%) carried canonical mutations in JAK2, 4/25 (16%) in CALR, and 4/25(16%) were triple negative.
Three patients each received 10 and 15 mg of RUX BD, 4 patients received 20 mg RUX BD, 21 patients received 25 mg RUX BD and 3 did not begin treatment. Median number of cycles received was 3 RUX and 4 AZA. The MTD of RUX in combination with AZA was determined at 25 mg BD, with no DLTs reported during phase 1 of the study. During the expansion phase, 1 DLT at dose level 3 was reported as grade 3 febrile neutropenia; with this patient's RUX dose reduced from 25 to 20 mg BD. Overall, 601 adverse events were reported of which 16.3% were grade 3 and 3.5% grade 4, with anaemia and febrile neutropenia the most common grade 3 and 4 events. There were 77 serious adverse events reported with 50.6% believed trial treatment related; febrile neutropenia, sepsis and, infections and infestations were the most common affecting 29.4%, 14.7% and 14.7% of patients respectively.
In total, 20 of 34 patients were evaluable for disease response. IWG MDS criteria were used for blasts <20% at baseline (Cheson Blood 2006), and Post MPN AML Consortium criteria for blasts ≥20% (Mascarenhas Leuk Res 2012). After 3 and 6 cycles the best responses achieved by MPN-AP patients were, 1 complete remission (CR), 4 marrow CR, 1 partial remission, 4 stable disease (SD), and 3 progressive disease. Best responses achieved by MPN-BP patients were, 4 acute leukaemia response-partial and 3 SD. The median response duration was 322 days for MPN-AP and 199 days for MPN-BP patients. Of the 14 RBC transfusion dependent patients at baseline, 0 and 3 (21.4%) of these achieved RBC transfusion independence after 3 and 6 cycles respectively. At baseline 7 patients were platelet transfusion dependent, 4 (57.1%) of these patients achieved platelet transfusion independence after 3 cycles and 1 (14.3%) persisted through 6 cycles. At 12 months the median PFS was 42.1% (95% CI: 17.9, 64.7), LFS was 26.4% (95% CI: 6.5, 52.2) and OS was 42.4% (95% CI: 23.8, 59.8).
Conclusions
The combination of RUX and AZA is well tolerated in MPN-AP and MPN-BP patients with toxicities comparable to the individual agents. Of evaluable patients 10 of 20 achieved a PR or CR. The OS compares favourably with historical cohorts and clinically meaningful responses were achieved for transfusion independence. In 1 patient the regimen permitted successful bridge to transplant. Such combinations should be further explored, potentially with higher dose RUX. An expanded molecular analysis including responses is presented as a separate abstract.
Drummond:Novartis: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding, Speakers Bureau; Gilead: Membership on an entity's Board of Directors or advisory committees; Takeda: Membership on an entity's Board of Directors or advisory committees; Blueprint Medicine Corporation: Research Funding; Jazz: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Bristol Myers Squibb: Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Astellas: Membership on an entity's Board of Directors or advisory committees; Pfizer: Consultancy, Membership on an entity's Board of Directors or advisory committees. Harrison:Shire: Honoraria, Speakers Bureau; Gilead Sciences: Honoraria, Speakers Bureau; Incyte Corporation: Speakers Bureau; Promedior: Honoraria; AOP Orphan Pharmaceuticals: Honoraria; CTI Biopharma Corp: Honoraria, Speakers Bureau; Novartis: Honoraria, Research Funding, Speakers Bureau; Celgene: Honoraria, Research Funding, Speakers Bureau; Sierra Oncology: Honoraria; Roche: Honoraria; Janssen: Speakers Bureau. Mead:Celgene/BMS: Consultancy, Honoraria, Other: travel, accommodations, expenses, Research Funding; Novartis: Consultancy, Honoraria, Other: travel, accommodations, expenses, Research Funding, Speakers Bureau; Gilead: Consultancy; CTI: Consultancy; Abbvie: Consultancy. Yap:Bristol-Myers Squibb: Honoraria, Speakers Bureau; Faron Pharmaceuticals: Consultancy. Narayanan:Takeda: Other: Educational support to attend conferences; Alexion: Speakers Bureau; MSD: Speakers Bureau; Celgene: Other: Educational support to attend conferences; Novartis: Other: Educational support to attend conferences. Somervaille:Novartis: Consultancy, Honoraria; Imago Bioscience: Research Funding. Gudgin:Jazz Pharmaceuticals: Membership on an entity's Board of Directors or advisory committees. Milojkovic:Incyte: Consultancy, Honoraria; Pfizer: Consultancy, Honoraria; Novartis: Consultancy, Honoraria; Bristol-Myers Squibb: Consultancy, Honoraria. Knapper:Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding.
5-azacitidine is licensed and approved for treatment of adult patients who are not eligible for HSCT with high risk myelodyplastic syndromes. Ruxolitinib is licensed and approved for use in Myelofibrosis and for Polycythaemia Vera resistant/intolerant to hydroxyurea

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal