

Introduction
Primary CNS lymphoma (PCNSL) is an aggressive form of lymphoid malignancy that occurs exclusively in the brain, meninges, spinal cord, and eyes. The incidence of PCNSL has been increasing, particularly in the elderly population, with a median age at diagnosis of 66 years (Olson J.E. et al., Cancer 2002). The primary modality of treatment for this deadly disease is systemic chemotherapy that includes high-dose methotrexate (HD-MTX), with or without whole-brain radiation. Due to the toxicity of HD-MTX, physicians tend to avoid using it in the elderly population. This was confirmed in previous reports from the 1990s (Panageas K.S. et al., Cancer 2007). In this comprehensive population-based analysis, we sought to examine the patterns of treatment and survival in elderly patients in the 2000s and sought to investigate clinical and socioeconomic predictors of treatment selection.
Methods
We conducted a retrospective cohort analysis using de-identified data accessed from the national cancer database (NCDB). The NCDB provided records of 2985 patients diagnosed with PCNSL between 2004 and 2015. We excluded patients who are younger than 65 years old, those who tested positive for HIV, and those who started treatment >120 days since diagnosis to account for immortal time bias. Patients were divided into four groups based on treatment received: combined modality treatment (CMT), chemotherapy alone, radiation alone, and no treatment. Exploratory analysis of the patient groups was performed. Summary statistics are presented as percentages for categorical data and median with interquartile range for quantitative data. Multivariate regression models were used to analyze predictors of the selection of any treatment versus no treatment and for selecting chemotherapy versus no chemotherapy. To account for variable baseline characteristics, we used propensity score weighting methodology to calculate estimates of interest. Survival estimates were performed using the Kaplan-Meier method, and survival differences were tested using the wilcoxon-rank test.
Results
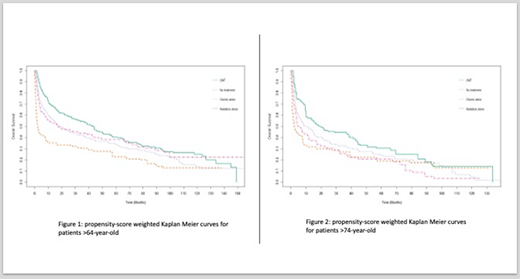
We identified 1096 patients with PCNSL who fulfilled the inclusion criteria. The median age was 73 (IQR: 68-79). There were 52% males. The majority of the patients were whites (92%), lived in a metropolitan area (78%), treated at an academic/research center (57%). The most common treatment modality used was chemotherapy alone (48%), followed by CMT (22%), no treatment (16%), and radiation alone (13%). On multivariate analysis, age (OR: 0.94, 95% CI 0.92-0.96) and comorbidity score (OR: 0.63, 95% CI 0.52-0.76) significantly predicted receiving any type of treatment. Both age (OR: 0.91, 95% CI 0.89-0.94) and distance (OR: 1.006, 95% CI 1.001-1.01) were predictors of receiving chemotherapy. Median follow up was 12 months (IQR: 3-44). Median OS in months for the four groups was: 43.1 for CMT, 19.4 for chemotherapy alone, 17.2 for radiation alone, and 2.3 for no treatment. (wilcoxon-rank test p-value: <0.001). Median OS for the whole population was 17 months (IQR: 12-26). Patients >75 year old had lower median OS in general, but receiving CMT had a survival advantage as well. (Figures 1 and 2)
Conclusions
The majority of PCNSL patients in our analysis received treatment. Our results showed an increased trend of chemotherapy use in elderly patients compared with earlier reports, where radiation alone was the most common treatment modality. The median OS of patients was longer compared with the 1990s data (17 vs. 7 months). CMT was associated with better OS compared with no treatment and chemotherapy alone. Although this was numerically better compared with radiation alone, it was not statistically significant. Younger patients and patients with lower comorbidity scores were more likely to receive treatment. Younger patients and patients who live further from the treating facility were more likely to receive chemotherapy. Longer distance may have led to less radiation use due to the need for complex planning and frequent visits associated with radiation therapy. Our study is limited by its retrospective nature, which makes it at risk of selection bias. Using propensity score weighting methodology strengthens our results. Also, the NCDB lacks certain pertinent variables, such as details of chemotherapy regimens, and toxicity information especially for radiation in the CMT arm which will have practical implications.
Fazal:Glaxosmith Kline: Consultancy, Speakers Bureau; Incyte Corporation: Consultancy, Honoraria, Speakers Bureau; Karyopham: Speakers Bureau; Celgene: Speakers Bureau; BMS: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Jansen: Speakers Bureau; Stemline: Consultancy, Speakers Bureau; Gilead/Kite: Consultancy, Speakers Bureau; Agios: Consultancy, Speakers Bureau; Amgen: Consultancy, Speakers Bureau; Takeda: Consultancy, Speakers Bureau; Novartis: Consultancy, Speakers Bureau; Jazz Pharma: Consultancy, Speakers Bureau. Kahn:Genetech: Honoraria; Takeda: Honoraria; Karyopharm: Honoraria; Seattle Genetics: Honoraria; Abbvie: Honoraria; Celgene: Honoraria; AstraZeneca: Honoraria; Beigene: Honoraria.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal