

Background: T follicular helper cells (Tfh), characterised by surface expression of CXCR5, PD1 and ICOS, regulate development of antigen-specific B cell immunity through germinal centre (GC) formation, generation of long-lived memory B cells and high-affinity plasma cells.
Methods: In this prospective study of peripheral blood B and circulating Tfh (cTfh) cell subsets, iTTP patients at 32 acute presentations, 23 elective rituximab (ER) episodes and 27 age & sex-matched healthy controls (HC) were studied using flow cytometry. All acute cases received PEX, steroids and RTX. All ER patients previously received RTX as acute therapy or previous ER at a median of 22 months (range 12-191 months). Serial samples were taken post-rituximab (RTX). B cell return was defined by laboratory CD19 count (<5 x 106/L). Statistical analysis was performed using GraphPad Prism 8.
Results: 11/32 (34%) acute cases received potentially immunomodulatory therapy prior to blood sampling and were excluded. Median ADAMTS13 activity was <5 IU/dL (<5-10.4 IU/dL) and anti-ADAMTS13 IgG 46% (2-127%). In 23 ER cases, median ADAMTS13 activity was 9 IU/dL (<5-24IU/dL) and antibody 8% (2-89%).
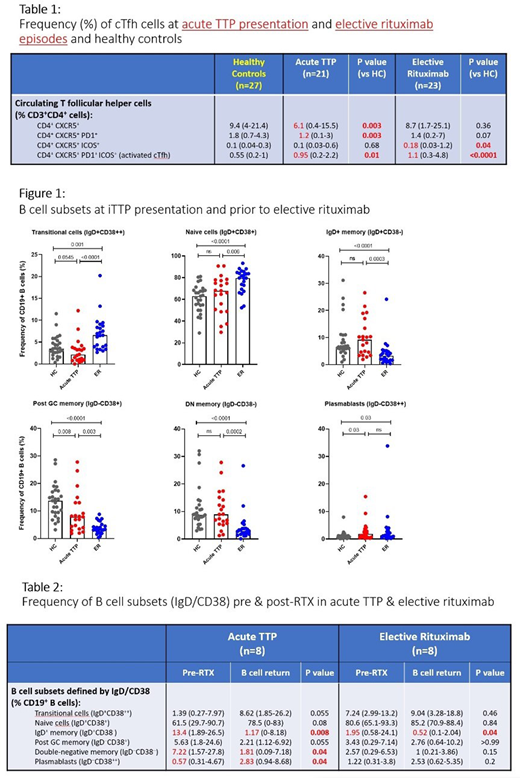
At acute presentation, CD4+CXCR5+ and CD4+CXCR5+PD1+ cTfh were decreased compared to HC (6.1% vs 9.4%; [p=0.003] and 1.2% vs 1.8%; [p=0.003] respectively), whereas activated cTfh (CD4+CXCR5+PD1+ICOS+) were increased (0.95% vs 0.55%; [p=0.01]) (Table 1).
B cell subsets in acute iTTP showed decreased pre-switch and switched memory subsets compared to HC: IgD+/CD27+ [p=0.003]; IgD-/CD27+ [p=0.02] and IgD-/CD38+ [p=0.008]. Plasmablasts (IgD-CD38++) were increased [p=0.03] (Figure 1).
ER patients pre-RTX had increased transitional and naïve B cells compared to HC [p=0.001; p<0.0001 respectively] and increased percentages of plasmablasts [p<0.0001]. Memory subsets defined by IgD/CD38 were all significantly decreased [p<0.0001] (Figure 1). Activated cTfh were increased in ER pre-RTX compared to HC [p<0.0001], whereas CD4+CXCR5+ICOS+ cells were reduced. There was no difference in CD4+CXCR5+ cells (Table 1).
Memory subsets (defined by IgD/CD38) in ER were all significantly reduced compared with acute iTTP cases (Figure 1) likely to be due to previously described (often long term) changes in B cell subsets following B cell return after RTX.
Longitudinal analysis: B cell return post-RTX in acute cases occurred mainly with transitional/naïve cells at a median of 8 months (0.5-14) but was not associated with iTTP relapse. Memory B cell subsets (defined by IgD/CD38) were significantly reduced at B cell return (Table 2). In ER patients, B cell subsets at repopulation were generally similar to levels seen prior to re-treatment with RTX. Frequency of cTfh was not significantly altered by RTX therapy in either acute TTP or ER.
Two ER patients were followed longitudinally from RTX therapy, through ADAMTS13 normalisation & subsequent fall requiring further RTX re-treatment. Asymptomatic ADAMTS13 relapse (activity <15 IU/dL) was temporally related with an apparent maturation to memory phenotype and increase in % plasmablasts.
Conclusions: At acute iTTP presentation and prior to elective re-treatment with RTX, activated (CD4+CXCR5+PD1+ICOS+) cTfh cells are increased, suggesting a role of T cell help in development of anti-ADAMTS13 IgG antibodies. Prior to RTX, B cell phenotype is also altered in acute TTP, with decreased frequency of memory subsets and a trend to increased naïve cells and plasmablasts. Persistent changes in B cell subsets were seen in ER patients who had received previous RTX with naive cells predominating and reduced memory cells. Interestingly, no patient relapsed/ required re-treatment related to B cell return, with relapse occurring at least 4 months after detection of B cells. Resumption of the autoimmune response therefore appeared limited by the rate of maturation of autoantigen(ADAMTS13)-specific B cells, either by selection/differentiation of ADAMTS13-naive B cells and/or expansion of ADAMTS13-specific memory B cells to Ig producing cells. This process, presumably driven by interaction with Tfh cells, suggests a role of T cell help in development of anti-ADAMTS13 IgG antibodies. Longitudinal analysis of the evolution of B and cTfh cells may help in predicting relapse in iTTP.
Scully:Alexion: Consultancy, Speakers Bureau; Ablynx/Sanofi: Consultancy, Other: Advisory Board, Speakers Bureau; Novartis: Other: Advisory Board, Speakers Bureau; Takeda: Consultancy, Speakers Bureau; Sanofi: Consultancy, Speakers Bureau; Takeda: Speakers Bureau; Shire/Takeda: Other: Advisory Board, Research Funding, Speakers Bureau. Thomas:Ablynx: Honoraria, Other: Advisory Board; Sanofi: Honoraria, Other: Advisory Board; Bayer: Honoraria, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal