


Background: The Platelet Function Analyser (PFA)-100 (Siemens) has proven to be a useful screening tool for primary hemostasis. Studies have demonstrated a pooled sensitivity around 90% for all individuals with Von Willebrand Disease (VWD), however the sensitivity for Type 1 is notably poorer than types 2 and 3. Our institution utilizes the PFA-100 as part of a panel of laboratory studies called the "bleeding screen"; this panel is often used as first line screening for inherited bleeding disorders across the hospital system. As the relative frequency of Type 1 VWD and low VWF (defined as Von Willebrand factor (VWF) levels 30-50%) greatly exceed the frequency of individuals with Type 2 and Type 3, when used as a general screen, the PFA-100 likely has reduced sensitivity than documented in the literature.
Methods: To evaluate the utility of the PFA-100 as a screening test for VWD and platelet function defects, we retrospectively examined the ordering practices of PFA-100 in relation to the Von Willebrand panel (VWF:antigen, VWF:ristocetin cofactor, Factor VIII), platelet aggregation studies and platelet electron microscopy. We compared results of the testing with diagnostic codes to characterize the test characteristics of the PFA-100 for the diagnosis of VWD or platelet function defects in a pediatric population. We included all patients tested with the PFA-100 from 2017 to 2018 at any Children's Healthcare of Atlanta facility. Exclusion criteria include age under 30 months (reference range established for those over 30 months), hematocrit <35% or platelets <150,000/uL at time of testing due to impact on PFA-100 results. Demographics, laboratory results, bleeding symptoms and diagnoses were collected via chart review. Bleeding disorders were determined by ICD-9 and ICD-10 codes and confirmed via chart review. Descriptive statistics were calculated with frequency and median (interquartile range); comparative statistics calculated with t-tests, chi-square, Fisher's Exact, Mann-Whitney and Spearman rank tests. Test characteristics for PFA-100 and VWD were determined by correlation between PFA-100 and VWD studies sent concurrently; a ristocetin co-factor <50% was considered positive for VWD in the comparative analysis. Test characteristics determined for platelet function testing were dependent on results of platelet aggregation studies and/or platelet electron microscopy.
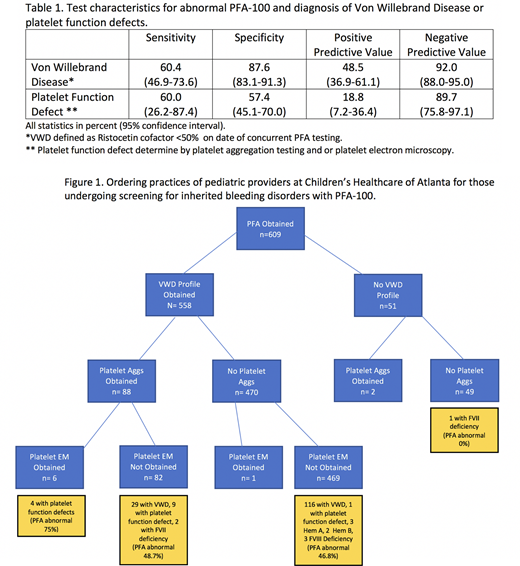
Results: There were 609 children who met inclusion criteria. Median age was 12.2 years (7.3-15.6). The majority were female (62.4%), white (58.5%) and non-Hispanic (77.0%). The most common reason for testing was epistaxis (28.1%), followed by heavy menstrual bleeding (24.8%) and bruising (18.4%). Almost 30% had no bleeding symptoms documented. The majority of individuals also had a VWD profile sent (91.5%), with 418 having the PFA-100 and VWD Profile sent concurrently. The majority of PFA-100 tests were normal (70.6%). Only 91 (14.9%) had additional platelet evaluation with platelet aggregation studies or electron microscopy. Overall, 170 individuals (27.9%) were found to have a bleeding disorder. VWD was diagnosed in 146 individuals (24.0%), a platelet function defect 14 (2.3%) and 11 individuals had other diagnoses including Factor VII deficiency, Hemophilia A and Hemophilia B. The sensitivity of the PFA-100 for VWD was 60.4% (95%CI 46.9-73.6%) and the sensitivity was 60.0% (26.2-87.4%) for platelet function defects. For those with an abnormal PFA, the results of a VWD profile did not determine the likelihood of a provider sending additional testing with platelet aggregation studies or platelet microscopy. Of the 104 individuals with an abnormal PFA and normal VWD studies, only 31 had platelet aggregation testing. There were no differences in demographics or reported symptoms between the two groups. With normal VWD studies, individuals with an abnormal PFA were about 3 times more likely to have platelet aggregation studies sent (p<0.0001).
Conclusion: The PFA-100 has poor sensitivity for VWD and mild platelet function defects in pediatric patients. Most individuals screened with a PFA-100 also had a complete VWD panel sent concurrently indicating that this is used as a screen for platelet function defects in our hospital. Given the poor sensitivity for platelet function defects, advanced platelet function testing should be sent based on clinical concern regardless of PFA-100 results when VWD testing is normal.
Brown:National Hemophilia Foundation, Takeda Clinical Fellowship: Research Funding. Woods:Takeda: Membership on an entity's Board of Directors or advisory committees.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal