

Introduction: Hematopoietic cell transplantation (HCT) is a standard therapy for patients with intermediate to high-risk acute myelogenous leukemia (AML), associated with improved long-term disease-free survival. Virginia is a diverse state, with rural and urban areas, including wealthy and disadvantaged counties. In this study, we compared HCT rates among different regions in the state of Virginia, and analyzed the impact of race/ethnicity, urban vs rural location, primary insurance payor, and socioeconomic status on access to HCT.
Methods: We conducted a retrospective, cohort study of patients age 18-75 diagnosed with AML in Virginia from 2013-2017 as reported to the Virginia Cancer Registry (VCR); the VCR was further linked with the Center for International Blood and Marrow Transplant Research (CIBMTR) database for identification of patients who had undergone HCT within two years of diagnosis. Socioeconomic data were generated from the VCR and the American Community Survey (ACS). Univariate and multivariable logistic regression models were used to examine several socioeconomic factors of interest, including patient-level information such as sex, age, race, marital status, primary insurance payor, and distance to closest transplant center as well as factors associated with geography, including specific regions (see Figure 1) and percentage of African Americans residing in the region (see Figure 2).
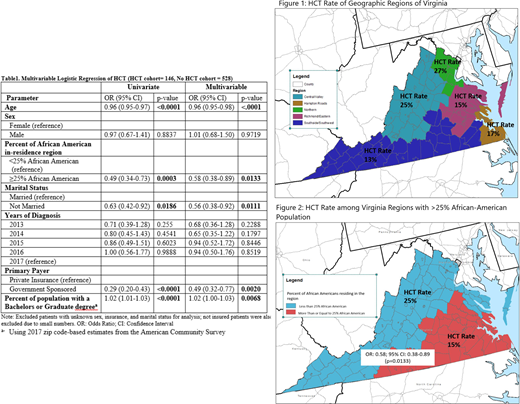
Results: There were 818 patients diagnosed with AML in Virginia from 2013-2017, and of these, 168 (21%) underwent HCT within two years of diagnosis. Median age was lower in the HCT cohort vs. the non-HCT cohort, 55 vs. 64 (p=<0.0001). There was a higher proportion of married patients in the HCT cohort vs. the non-HCT cohort, 67% vs. 53% (p=0.005). The rate of HCT varied by geographic region (p=0.004; see Figure 1). The univariate and multivariate analyses (see Table 1) showed decreased likelihood of HCT with increasing age (OR: 0.96; 95% CI: 0.95-0.98). Patients from regions which had greater than 25% African American population were 42% less likely to undergo HCT (OR: 0.58; 95% CI: 0.38-0.89) (see Figure 2). Patients who were not married were less likely to undergo HCT compared to married patients (OR 0.56; 95% CI: 0.38-0.92). Patients with government insurance as primary payor were less likely to undergo HCT compared to patients with private insurance (OR 0.49; 95% CI: 0.32-0.77). Patients living in areas (by zip code) with a greater percentage of population with a college/graduate degree were more likely to undergo transplant than the patients living in areas with a lower percentage of college/graduate degree (OR: 1.02; 95% CI: 1.00-1.03).
Conclusion: From 2013-2017, only 21% of patients with AML in Virginia underwent HCT within two years of diagnosis. We found that the likelihood of undergoing HCT is associated with age, percent of African Americans residing in the region, marital status, primary insurance payor, and percent of population with a bachelor or graduate degree. Our findings suggest geographic and socioeconomic factors are likely barriers to access to HCT. The decreased rate of HCT in regions with a higher percent of African-Americans may reflect structural racism, both due to factors outside and within the medical community. Resources should be devoted to specific interventions addressing disadvantaged populations, including early human leukocyte antigen (HLA) typing, caregiving resources, increased diversity of donor pool, and improved insurance coverage. Future studies will evaluate access to HCT after referral to HCT centers as well as racial disparity in access to HCT across the United States.
Balkrishnan:Merck and Co.: Consultancy. Devine:Magenta Therapeutics: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal