

Background: In addition to efficacy and safety, patient and healthcare professional (HCP) experiences are important aspects of treatment selection. Daratumumab (DARA) is a humanized monoclonal antibody targeting CD38 and is approved as monotherapy or in combination with standard of care regimens for the treatment of multiple myeloma (MM). Administration of DARA intravenous (IV) takes approximately 7 hours for the first infusion and 3-4 hours for subsequent infusions. To reduce this burden, DARA subcutaneous (SC; DARA 1800 mg coformulated with recombinant human hyaluronidase PH20 [rHuPH20; 2000 U/ml; ENHANZE® drug delivery technology, Halozyme, Inc., San Diego, CA, USA]) was developed. In the phase 3 COLUMBA trial (NCT03277105), at a median follow-up of 7.5 months, overall response and maximum trough concentration with DARA SC were noninferior to DARA IV in patients with relapsed/refractory MM (RRMM). Based on these results, DARA SC was approved by the Food and Drug Administration and European Medicines Agency.
Based on an SC injection duration of 5 minutes, administration of DARA SC injections is estimated to take <2 hours (115 minutes) of HCP time during the first year of treatment. A time and motion survey was undertaken to elicit HCPs' understanding of workflow and time estimates for administration of DARA IV and SC (beyond injection time alone) in patients with RRMM. Data collection was halted due to the COVID-19 pandemic. Here, we report the interim survey results.
Methods: A web-based, prospective survey was designed to collect primary data from HCPs at sites that actively enrolled patients in the COLUMBA trial.
Data were collected for DARA IV and SC regarding time spent on prespecified drug preparation and drug administration/patient care activities; for each task, the respondent's perception of average time and HCP who performs the task were captured. Patient data, including efficacy and safety information, were not collected.
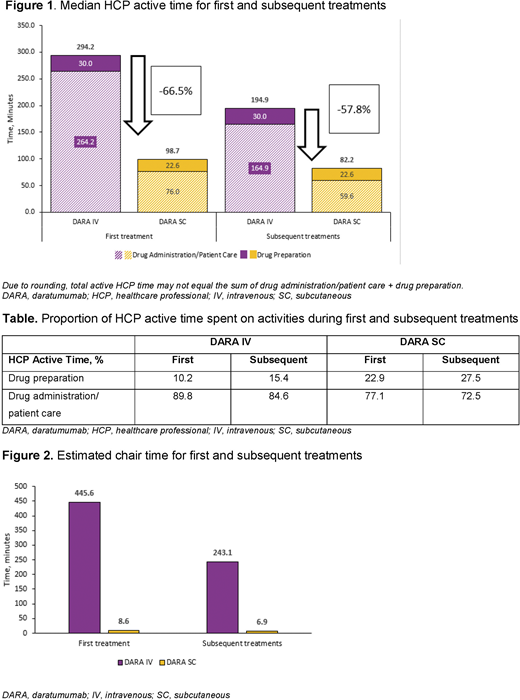
The primary endpoints are mean and median active HCP time for each prespecified activity. Time for each activity was adjusted by its probability of occurring (eg, management of infusion-related reactions). Median results are reported here, as these are considered a better measure of central tendency than the mean. Total median active HCP time was calculated by summing median time for all prespecified activities (drug preparation activities vs activities in the patient care area/infusion suite). A post-hoc analysis estimated patient chair time based on HCP inputs for pre-treatment activities, infusion/injection duration, and post-treatment activities. A sensitivity analysis was conducted comparing a subgroup of respondents with fully validated data with the overall study population.
Results: A total of 26 respondents from 8 countries (Brazil, Israel, Japan, Greece, Poland, Sweden, Taiwan, and Ukraine) completed the survey. For DARA IV, the median total active HCP time was 294.2 minutes for the first infusion and 194.9 minutes for subsequent infusions (Figure 1). For DARA SC, the median total active HCP time was 98.7 minutes for the first injection (66.5% reduction in time vs DARA IV) and 82.2 minutes for subsequent injections (57.8% reduction in time vs DARA IV) (Figure 1). For both treatments, the proportions of time spent on drug preparation vs drug administration/patient care were roughly similar for first and subsequent administrations (Table). When extrapolated for year 1 and year 2 (23 administrations in year 1 and 13 in year 2, as per label), estimated active HCP time per patient was 76.4 and 42.2 hours, respectively, for DARA IV and 31.8 and 17.8 hours, respectively, for DARA SC. Estimated chair time for DARA IV was 445.6 minutes for the first infusion and 243.1 minutes for subsequent infusions; for DARA SC, estimated chair time for first and subsequent injections was 8.6 and 6.9 minutes, respectively (Figure 2). Results were confirmed by a sensitivity analysis using fully validated data for 13 of the 26 respondents.
Conclusions: Results of this time and motion survey indicate that DARA SC is associated with less active HCP time spent on drug preparation and drug administration/patient care compared with DARA IV. This reduced treatment burden may translate into advantages for patients (less time away from home, family, and/or work) and efficiencies for HCPs and healthcare facilities (ability to treat a greater number of patients).
Slavcev:Janssen: Current Employment. Spinelli:Janssen: Current Employment. Absalon:Syneos Health: Current Employment. Masterson:Janssen: Current Employment. Heuck:Janssen: Current Employment. Lam:Janssen: Current Employment. De Cock:Syneos Health: Current Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal