

COVID-19 is a severe infectious complication in patients with underlying medical conditions such as having undergone hematopoietic stem cell transplantation (HCT). This prospective survey reports outcome on 272 COVID-19 patients from 19 countries having undergone allogeneic (n = 175) or autologous (n = 97) HCT reported to the EBMT registry or to the GETH. All patients had the diagnosis of SARS-CoV-2 documented by PCR. Patients were included in this analysis if COVID-19 diagnosis was before April 10, 2020. The overall survival was estimate by using the Kaplan Meier methods, considering the death due to any cause as an event and the time from COVID-19 infection to the latest follow-up as survival time; difference between groups were tested by the log-rank test. Univariate and multivariate risk factor analysis for overall survival were performed with the Cox regression model.
The median age was 54.4 years (1.0 - 80.3) for allogeneic and 60.9 years (7.7 - 73.4) for autologous HCT patients. 20 patients were children (< 18 years of age; median age 11.3 (1.0 - 16.9)). The median time from HCT to diagnosis of COVID-19 was 13.7 months (0.2 - 254.3) in allogeneic and 25.0 months (-0.9 - 350.3) in autologous recipients. Lower respiratory tract disease (LRTD) developed in 84.8% and 21.5% were admitted to an intensive care unit (ICU). At the time of analysis, 68/238 (28.6%) patients had died (47/155 allogeneic patients; 21/83 autologous patients). No follow-up had been received on 34 patients. The median time from infection to death was 19 days (0-102). Five patients were reported to have other primary causes of death than COVID-19. Of the patients reported to be alive, the median follow-up was 44 days. 144 (84.7%) patients (93 allogeneic; 51 autologous) had virologic resolution of the COVID-19 infection having at least one negative PCR. 26 patients were alive and known to be still COVID-19 positive (15 allogeneic; 11 autologous). For 34 patients the resolution status was unknown. Factors influencing the likelihood of resolution in multivariate analysis were underlying diagnosis (p=.01) and longer time from transplant to diagnosis of COVID-19 (p=.035).
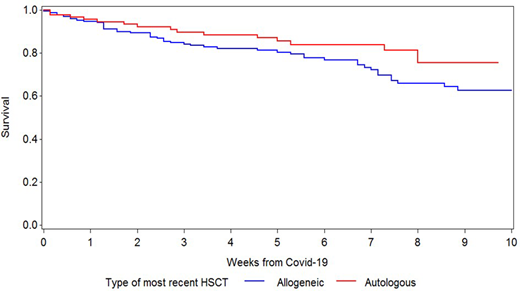
Overall survival at 6 weeks from COVID-19 diagnosis was 76.8% and 83.8% in allogeneic and autologous HCT recipients (p =ns), respectively (figure 1). Children (n=20) tended to do better with a 6-week survival of 95.0% although the difference was not significantly different (p =.12). In multivariate analysis of the total population older age (HR 1.26; 95% CI 1.05 - 1.51; p = .01) increased the risk and better performance status decreased the risk for fatal outcome (HR 0.79; 95% CI 0.69 - 0.90; p = .0003). The same factors had significant impact on overall survival in allogeneic HCT recipients (age HR 1.28; 95% CI 1.05 - 1.55; p=.01; performance status HR 0.79; 95% CI 0.68 - 0.92); p=.002) while only age impacted survival among autologous HCT patients (data not shown). Other transplant factors such as underlying diagnosis, time from HCT to diagnosis of COVID-19, graft-vs-host disease, or ongoing immunosuppression did not have a significant impact on overall survival.
We conclude that HCT patients are at an increased risk compared to the general population to develop LRTD, require admission to ICU, and have increased mortality in COVID-19.
Duarte:Incyte Corporation: Other: Has received speaker and advisor fees. Kwon:Jazz: Consultancy, Honoraria; Gilead: Consultancy, Honoraria; Novartis: Consultancy, Honoraria; Pfizer: Consultancy, Honoraria. Mielke:Novartis: Honoraria, Other: received via my institution, Speakers Bureau; Celgene/BMS: Honoraria, Other: received via my institution , Speakers Bureau; Bellicum: Honoraria, Other: received via my institution, Speakers Bureau; Kite/Gilead: Honoraria, Other: received via my institution , Speakers Bureau; Miltenyi: Honoraria, Membership on an entity's Board of Directors or advisory committees, Other: received via my institution , Speakers Bureau; KIADIS Pharma: Honoraria, Other: received via my institution , Speakers Bureau; DNA Prime: Honoraria, Other: received via my institution , Speakers Bureau. López Jiménez:MSD: Speakers Bureau; Roche: Research Funding, Speakers Bureau; Takeda: Speakers Bureau; Janssen: Research Funding, Speakers Bureau; Abbvie: Research Funding, Speakers Bureau; Gilead: Research Funding, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal