

INTRODUCTION
Heavy menstrual bleeding (HMB) is one of the most common disease manifestations of biological females with inherited bleeding disorders and is often accompanied by iron deficient anemia (IDA). The most common bleeding disorders identified in biological females are von Willebrand Disease (VWD)/low von Willebrand Factor levels (low VWF) and heterozygosity for factor VIII genetic defects. Several pre-analytical variables including elevated adrenergic stress and estrogen-states can make it challenging to accurately diagnose these conditions as these variables are known to influence VWF and factor VIII activity levels. We sought to investigate whether an iron depleted state impacts the results of a laboratory assessment for VWD/low VWF or mild hemophilia A.
METHODS
Subjects were recruited from the Spots and Dots clinic (female-identifying bleeding disorder clinic) through the University of Colorado's Hemophilia and Thrombosis Center. Eligible subjects included biological females of any age who had at least two sets of laboratory assessments for von Willebrand levels (VWF antigen, VWF activity, and factor VIII activity level) and markers for total body iron stores (complete blood count and ferritin). Age at time of first testing, iron prescriptions, and underlying bleeding disorder diagnoses were also recorded. IDA was defined as a ferritin less than 20ng/mL with accompanying anemia (Hb <14.3 g/dL). Descriptive statistics and Fisher's exact tests were used to evaluate the association of factor VIII/VWF activity levels and iron stores.
RESULTS
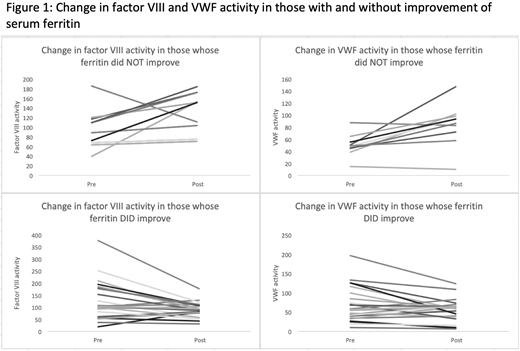
Thirty-seven subjects were included in the final analysis. The average age at time of first testing was 21.5 years (range 9-50 years). IDA was present in 22 patients at the time of first assessment and in 20 patients at follow up. Serum ferritin improved overall in 23 patients between assessments. Oral iron was prescribed in 20 patients and intravenous iron was prescribed in three. An improvement in serum ferritin predicted a decrease in factor VIII activity (p = 0.0092) on follow-up assessment but did not predict a significant decrease in VWF activity levels (p = 0.0819) (Figure 1). Retesting factor VIII and VWF activity levels after iron repletion led to a diagnosis of low VWF in 4 cases (10.8%) and VWD in 2 cases (5.4%) that would have otherwise been classified as normal without retesting.
CONCLUSIONS
IDA is frequent in women with HMB and may be insufficiently managed with oral iron therapy in adolescents and those with an underlying bleeding disorder. The fact that many patients remained iron deficient at the time of follow up testing may have blunted the results of this analysis. Despite this limitation, this study still suggests that iron deficient anemia may be a significant enough biological stressor to increase factor VIII and possibly VWF activity levels to a point that may obscure an underlying diagnosis of VWD, low VWF, or hemophilia A. Further investigations are warranted to confirm if universal retesting of VWF and factor VIII activity levels are diagnostically imperative after correction of IDA. Such a recommendation may have a significant impact on this patient population as discovery of an underlying bleeding disorder diagnosis can not only provide an explanation for a patient's HMB but also can identifying individuals who may be at increased risk for bleeding at other sites or during invasive procedures.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal