

Introduction.
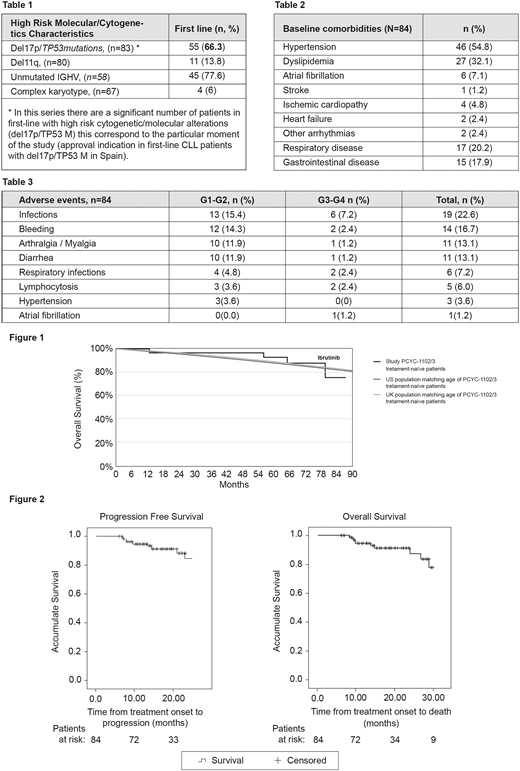
Ibrutinib is a first-in-class, oral, once-a-day Bruton's tyrosine kinase inhibitor that achieves high overall response rates and durable remissions in patients with chronic lymphocytic leukemia (CLL) including those with high-risk features (unmutated IGHV, TP53 abnormalities, 11q deletion). Survival with continuous single-agent ibrutinib in previously-untreated CLL patients is comparable to an age-matched general population (Figure 1). IBRORS is an observational, retrospective, multicentre study to describe the characteristics and clinical outcomes of patients with CLL treated with single-agent ibrutinib in routine clinical practice in Spain. This present analysis reviews the subset of patients in IBRORS who received ibrutinib as the first-line of treatment. This series includes a significant number of patients with high risk cytogenetic/molecular alterations (del17p/TP53 M), which corresponds with the approved indication for first-line CLL patients in Spain at the time.
Methods.
Adult patients diagnosed with CLL treated with single-agent ibrutinib in first-line, or at first or second relapse since its commercialization in Spain (between January 2016 to January 2019) were included in the IBRORS study. Clinical characteristics of patients, efficacy and tolerability of ibrutinib as first-line treatment were analyzed here. A Kaplan-Meier analysis was performed for overall survival (OS) and progression-free survival (PFS).
Results.
84 patients, from a total of 269 included in IBRORS, received single-agent ibrutinib as first-line treatment. The median age was 71.3 years (range 63-77) at the time of ibrutinib initiation. 56.3% of patients presented with an intermediate/high-risk Rai-Binet stage, and the majority of patients (98.6%) had an ECOG PS of 0-1. 91.7% of patients had at least 1 high risk molecular cytogenetic factor (unmutated IGHV, TP53 abnormalities, 11q deletion or complex karyotype) described in table 1.
Baseline comorbidities of patients are described in table 2. Concomitant medication included anticoagulants (9.5% patients; vitamin K antagonist [n=4], Apixaban [n=1] and LMWH [n=3] patients), antiplatelet agents (11.9% patients), and antihypertensives (50% patients).
The overall response rate (ORR) was 79.5%; 14/84 (16.6%) achieved a complete response (CR), 14/84 (16.6%) achieved CR unconfirmed, 27/84 (32.14%) achieved a partial response (PR) and 12/84 (14.2%) a PR + lymphocytosis. The median PFS and OS were not reached, and the estimated PFS at 24 months was 84.5% (73.4-95.6%). OS and PFS curves are represented in figure 2.
The PFS of each patient subgroup with high-risk cytogenetic characteristics was similar to that of all patients in the first-line cohort: del17p/TP53 mutation (HR = 0.963 [95% CI 0.188-4.928]; p = 0.964), del11q (HR = 0.042 [95% CI 0.000-682.736]; p=0.521), unmutated IGHV (HR = 0.391 [95% CI 0.110-1.394]; p = 0.148).
The median duration of exposure to ibrutinib was 17.3 (11.9-25.6) months. Dose reduction of ibrutinib occurred in 17/84 (20.2%) patients, 8/84 (9.52%) due to toxicity (4 hematologic toxicity and 4 non-hematologic toxicity). 27/84 (32.1%) patients had temporary interruption of treatment. 15/84 (17.8%) patients permanently discontinued ibrutinib including 6 (7.14%) patients due to progression, 4 (4.76%) due to toxicity and 5 for other reasons.
Safety:
49/84 (58.3%) patients developed at least one adverse event (AE), while 12/84 (14.2%) patients developed at least one serious adverse event (SAE). Twelve (14.3%) patients reported at least one haematological toxicity while 53 patients (63.1%) recorded at least one non-haematological toxicity. Only 1 patient experienced grade 3 atrial fibrillation, which did not lead to discontinuation. The most common AEs are described in table 3.
Conclusion.
This population of previously-untreated CLL patients, enriched for high-risk genomic features, reflects the initial approval of ibrutinib for the treatment of first-line patients with del17p in Spain. Single-agent Ibrutinib as the first-line treatment in this real world population was effective regardless of risk factors and well tolerated, with a low rate of discontinuation due to toxicity. Findings are consistent with those reported in clinical trials.
Loscertales:AbbVie: Honoraria, Membership on an entity's Board of Directors or advisory committees; Janssen: Honoraria, Membership on an entity's Board of Directors or advisory committees; AstraZeneca: Membership on an entity's Board of Directors or advisory committees; Roche: Honoraria. Arguiñano:AbbVie: Honoraria; Janssen: Honoraria; BMS-Celgene: Honoraria; Novartis: Honoraria. Hernandez-Rivas:Janssen: Membership on an entity's Board of Directors or advisory committees; Abbvie: Membership on an entity's Board of Directors or advisory committees; Roche: Membership on an entity's Board of Directors or advisory committees; AstraZeneca: Membership on an entity's Board of Directors or advisory committees; Gilead: Membership on an entity's Board of Directors or advisory committees; Celgene/BMS: Membership on an entity's Board of Directors or advisory committees; Rovi: Membership on an entity's Board of Directors or advisory committees. Pérez Persona:Amgen: Consultancy; Celgene: Consultancy, Speakers Bureau; Roche: Consultancy, Speakers Bureau; Jannsen: Consultancy, Speakers Bureau; Abbvie: Consultancy, Speakers Bureau; Takeda: Consultancy. Loriente:Janssen Cilag: Current Employment. Villanueva:Janssen Cilag: Current Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal