

Introduction:
Multiple myeloma (MM) is an incurable malignancy, and clinical trials with newer agents have shown improved patient outcomes. Ixazomib (Ixa) is a proteasome inhibitor and induces apoptosis in cancer cells. It is commonly used with immunomodulators for the treatment of MM. We conducted a systematic review and meta-analysis to assess the efficacy of Ixazomib alone and in combination with other drugs for the treatment of newly diagnosed multiple myeloma (NDMM).
Methods:
A literature search was performed on PubMed, Cochrane, Embase, Web of Science, and clinicaltrials.gov. We used the following MeSH and Emtree terms; "ixazomib" AND "Multiple Myeloma" from inception till 06/05/2020. We screened 1,558 articles and included 3 randomized clinical trials (RCTs) (N=901) and 12 non-randomized clinical trials (NRCT) (N=632). We excluded case reports, case series, preclinical trials, review articles, observational studies, meta-analysis, and ongoing clinical trials that did not report interim efficacy outcomes. We used the R programming language (version 4.0.2) to conduct a meta-analysis.
Results:
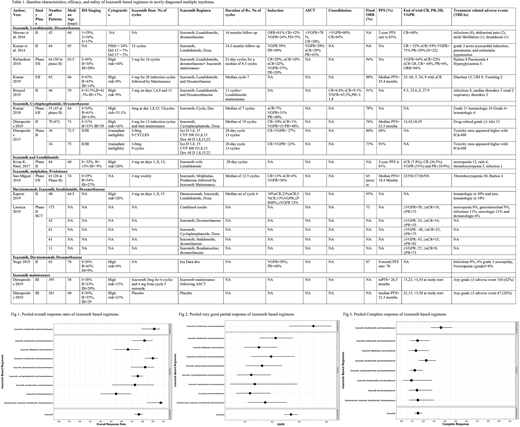
In 15 clinical trials (N=1533), Ixa based regimens were used in patients with age range of 39-92 years. (Table 1) In 3 clinical trials (N=170), Ixa with Lenalidomide (Len) and dexamethasone (Dex) yielded a pooled overall response rate (ORR) of 90% (95% CI=0.82-0.94, I2=32%), a pooled complete response (CR) of 23% (95% CI=0.16-0.32, I2=24%) and a pooled ≥very good partial response and better (≥VGPR) of 39% (95% CI=0.24-0.57, I2 =76%) when used as induction therapy for NDMM patients. As consolidation therapy (N=88), pooled ORR was 91% (95% CI=0.79-0.97, I2=0), pooled CR was 36% (95% CI=0.27-0.47, I2=0) and pooled ≥VGPR was 70% (95% CI=0.53-0.84, I2=60%). (Fig 1-3)
In 5 clinical trials (N=233), Ixa + cyclophosphamide (Cyc) + Dex yielded a pooled ORR, CR, and ≥VGPR of 76% (95% CI=0.70-0.81, I2 =0), 12% (95% CI=0.07-0.20, I2=44%), and 25% (95% CI=0.14-0.39, I2=78%), respectively. (Fig 1-3) The lower dose of Cyc 300mg/m2 had similar efficacy as 400mg/m2 with better safety profile in elderly patients. In a RCT (N=175) of Ixa with multiple combinations, Ixa + Dex yielded ORR 55% (95% CI=0.40-0.69), CR 14% (95% CI=0.07-0.28) and ≥VGPR 24% (95% CI=0.13-0.39). Ixa+ thalidomide (Thal) + Dex fostered ORR 82% (95% CI=0.70-0.90), CR 15% (95% CI=0.08-0.26), and VGPR 43% (95% CI=0.31-0.55). Ixa + bendamustine + Dex yielded ORR of 73% (95% CI=0.41-0.91), CR 9% (95% CI=0.01-0.44), and ≥VGPR 27% (95% CI=0.09-0.59). In one clinical trial (N=53), Ixa + melphalan (Mel) + prednisone (Pred) combination yielded pooled ORR, CR, and ≥VGPR of 66% (95% CI=0.52-0.77), 13% (95% CI=0.06-0.25), and 30% (95% CI=0.19-0.44), respectively. In a phase II trial (N=40), Ixa + daratumumab (Dara) + Len + Dex yielded an ORR, CR and ≥VGPR of 97% (95% CI=0.84-1), 15% (95% CI=0.07-0.28), and 35% (95% CI=0.22-0.51) respectively. (Fig 1-3)
In a phase III RCT by Dimopholous et al. (N=656), Ixa maintenance therapy after stem cell transplant (SCT) yielded an ORR, CR, and ≥VGPR of 76%, 15%, and 54%, respectively. They observed 28% reduction in the risk of progression or death with Ixa vs. placebo, median progression free survival (mPFS) was 26.5 months (95% CI 23·7‐33·8) vs 21·3 months [18·0‐24·7]; hazard ratio 0·72, 95% CI 0·58‐0·89; p=0·0023). Second malignancies were 3% in both ixazomib and placebo group. 27% of the patients in ixazomib group and 20% patients in placebo group experienced serious adverse events.
In a clinical trial on unfit and frail patients (N=46) treated with Ixa + daratumumab (Dara) + Dex, pooled ORR and ≥VGPR were 83% (95% CI=0.69-0.91, I2=0), and 33% (95% CI=0.21-0.47, I2=0), respectively. (Fig 1-3) In the phase II trial, ORR, CR, and VGPR with ixazomib and lenalidomide were 64%, 26%, and 53%, respectively.
Conclusion:
Ixa in combination with Len, Dex, Cyc, Dara, Mel, Pred is effective in the treatment of NDMM patients. In early phase trials, Ixa with Dara, Len, and Dexa showed the highest overall response as induction therapy. Ixazomib maintainance therapy prolongs PFS after SCT as compared to placebo and represents an additional option for post SCT maintainace therapy in NDMM patiens. The safety profile of Ixa was acceptable with most commonly encountered adverse events were hematological including neutropenia and thrombocytopenia. Additional multicenter, double-blind, randomized clinical trials are needed to confirm these results.
Anwer:Incyte, Seattle Genetics, Acetylon Pharmaceuticals, AbbVie Pharma, Astellas Pharma, Celegene, Millennium Pharmaceuticals.: Honoraria, Research Funding, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal