

Background:
Randomized trials in the pre-rituximab era showed that watch and wait (WW) when compared to initial treatment (IT) for asymptomatic advanced-stage follicular lymphoma (FL) did not impact overall survival (OS). In the rituximab era, a randomized trial showed patients with advanced-stage, asymptomatic, low-burden FL were less likely to need chemotherapy at 3 years when treated with rituximab only at diagnosis compared to WW, however with no difference in OS (Ardeshna et al., 2014). In another analysis, there was no impact of WW compared to IT on the time to next anti-lymphoma therapy (Solal-Celigny et al., 2012). However, the existing studies were limited by sample sizes and not powered by survival. In addition, few patients with grade 3a FL were included, thus it is not clear if pathological grades (other than grade 3b) should be taken into consideration when choosing WW vs IT.
Here we studied the outcomes of WW vs IT for patients with advanced-stage (stage III/IV) FL using the National Cancer Database (NCDB) and compared the outcomes by FL pathological grades.
Methods:
Patients diagnosed between 2011-2016 were included. We only included patients diagnosed after 2011 (when rituximab was FDA approved for FL as maintenance) so our results reflect the current management of FL. To ensure accurate reporting of IT, only patients who were diagnosed and initially managed at the reporting facility were included. Demographic characteristics were compared using Chi-square test for categorical variables and ANOVA for continuous variables. Univariate comparison of OS was conducted using Logrank test. Multivariate survival analysis was conducted using Cox proportional hazard model with the following covariates: age, gender, race, Hispanic ethnicity, stage, grade, existence of previous malignancies, comorbidity score, facility type, facility lymphoma patient volume, urban/rural location, education, income and insurance status.
Results:
A total of 14417 patients with stage III/IV FL were included. Among them, 10755 received IT (74.6%) and 3662 (25.4%) were managed by WW at diagnosis. For those who received IT, the median time to treatment was 35 days (IQR 22-56 days).
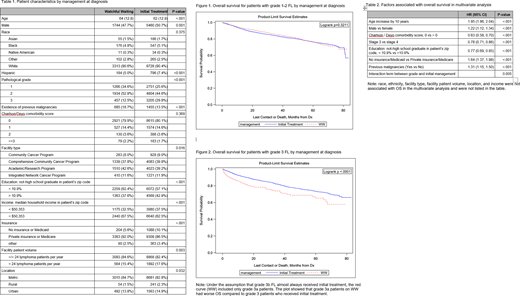
Preliminary analyses showed that patients with grade 1 FL and grade 2 FL were managed similarly and had similar OS, therefore we combined grade 1 and grade 2 into grade 1-2 FL as opposed to grade 3 FL.
A total of 13050 patients had grade 1-2 FL and 4286 patients had grade 3 FL. Patients with grade 1-2 FL were more likely to be managed by WW than those with grade 3 FL (29.8% vs 12.5%, respectively; p<0.01).
Patients on WW were older, more likely to be female, more likely to have previous malignancies, had higher education and income, and more likely to have private insurance or Medicare than Medicaid or no insurance (Table 1).
Patients with grade 1-2 FL had similar OS when managed by WW compared to IT (5-year OS rate: 76.3% vs 76.2%, respectively; p=0.32; Figure 1). In contrast, patients with grade 3 FL had worse OS when managed by WW compared to IT (5-year OS rate: 65.3% vs 73.5%; p<0.001; Figure 2). In multivariate analysis, the interaction term between grade and management was significant (p=0.005), confirming that initial management affected OS in different ways for grade 1-2 FL and grade 3 FL after adjusting for the covariates. Consistent with the results of the univariate analysis, after adjusting for covariates, grade 1-2 FL had similar survival when managed by WW compared to IT (HR=0.93, 95% CI: 0.82-1.05; p=0.25) but grade 3 FL had worse survival when managed by WW (HR=1.43, 95% CI: 1.14-1.82; p=0.002).
Other factors associated with OS are listed in Table 2.
Conclusion:
Our study confirms the findings of lack of OS benefits in patients with advanced stage, grade 1-2 FL when treated with WW versus IT. In contrast, patients with advanced stage, grade 3 FL had worse OS with WW approach. While the NCDB does not separate grade 3 FL into 3a and 3b, it is assumed that FL 3b is universally managed as DLBCL and receive IT given its more aggressive course. Under this assumption, all grade 3 FL patients on WW were likely grade 3a. Thus, our results suggest that grade 3a FL patients on WW had worse OS compared to grade 3 FL patients who received IT (see Figure 2 and its footnote for illustration). Although a definitive conclusion cannot be made regarding grade 3a FL, further studies to compare the outcome of WW vs IT with special focus on stage 3a FL are warranted.
Shah:NCCN: Vice-Chair, Acute Lymphoblastic Leukemia Working Group: Membership on an entity's Board of Directors or advisory committees; Kite/Gilead, Precision Biosciences, Novartis, AstraZeneca: Other: TRAVEL, ACCOMMODATIONS, EXPENSES; Kite/Gilead, Celgene/Juno/BMS, Novartis, Pfizer, Amgen, Spectrum/Acrotech, Precision Biosciences, Beigene, AstraZeneca, Pharmacyclics/Jansen, Adaptive: Honoraria; Moffitt Cancer Center: Current Employment; Kite/Gilead, Jazz, Incyte: Research Funding. Bello:Seattle Genetics: Consultancy, Honoraria, Speakers Bureau; Celgene: Consultancy, Honoraria, Speakers Bureau. Sokol:EUSA Pharma: Consultancy, Honoraria, Speakers Bureau; Kymera Therapeutics: Membership on an entity's Board of Directors or advisory committees; Kyowa/Kirin Inc.: Membership on an entity's Board of Directors or advisory committees. Pinilla Ibarz:Pharmacyclics: Consultancy, Speakers Bureau; Novartis: Consultancy; Sanofi: Consultancy; TG Therapeutics: Consultancy; Janssen: Consultancy, Speakers Bureau; Sunesis Pharmaceuticals: Consultancy; AstraZeneca: Consultancy, Speakers Bureau; Takeda: Consultancy, Speakers Bureau; Abbvie: Consultancy, Speakers Bureau. Chavez:Karyopharm: Consultancy; BeiGene: Speakers Bureau; Bayer: Consultancy; Merck: Research Funding; Morphosys: Consultancy, Speakers Bureau; AstraZeneca: Speakers Bureau; Celgene: Consultancy; Novartis: Consultancy; AbbVie: Consultancy; Genentech: Speakers Bureau; Epizyme: Speakers Bureau; Gilead: Consultancy; Kite, a Gilead Company: Consultancy, Speakers Bureau; Verastem: Consultancy; Pfizer: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal