

Introduction
Cold agglutinin disease (CAD) is a serious and rare autoimmune hemolytic anemia driven by cold agglutinin autoantibodies, which bind to red blood cells and activate the classical complement system to initiate hemolysis and anemia (Berentsen S. Hematology Am Soc Hematol Educ Program 2016). There is limited evidence on the individual and societal impact of CAD. A retrospective study of 27 patients in a US healthcare institute demonstrated fluctuations in severity of anemia over the course of the disease, and significant utilization of healthcare resources (Mullins M et al. Blood Adv 2017). The objective of this study was to understand the long-term characteristics and disease burden in patients with primary CAD from a large US Electronic Health Record (EHR) database.
Methods
This retrospective observational cohort study included adult patients from the Optum© EHR database between January 1, 2007 and September 30, 2019 who had ≥1 medical encounter with an autoimmune hemolytic anemia-related diagnosis code, ≥3 documentations (on different dates) of CAD and ≥1 hemoglobin (Hb) value <12 g/dL. The index date was defined as the first mention of CAD; all patients were required to have a 12-month baseline period prior to this. To limit the study to patients with primary CAD, patients were excluded if they had ≥1 medical encounter with mycoplasma, cytomegalovirus and Epstein-Barr at the index date, or ≥1 medical encounter with lymphoma, MALT lymphoma, chronic lymphoid leukemia, Waldenstrom macroglobulinemia or myeloma during the baseline period.
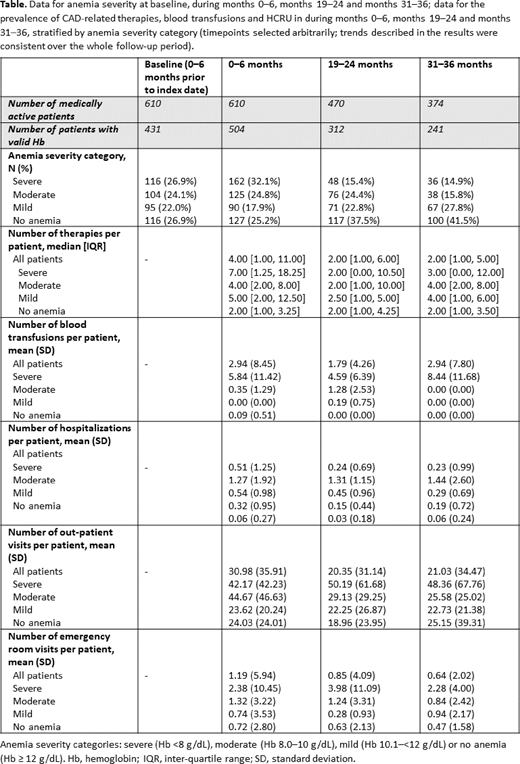
Anemia severity (defined as the lowest Hb value in each study period), utilization of CAD-related therapies, blood transfusions and all-cause healthcare resource utilization (HCRU) were analyzed at baseline and at 6-month follow-up intervals. Although no treatment is approved in CAD, corticosteroids, immunoglobulin, rituximab, immunosuppressants, antineoplastic and biologics were considered as CAD-related therapies to reflect usual practice. Results were stratified by anemia severity category (severe [Hb <8 g/dL], moderate [Hb 8.0-10 g/dL], mild [Hb 10.1-<12 g/dL] or no anemia [Hb ≥12 g/dL]) during each follow-up interval. Severe hemolysis was defined as elevated LDH and/or elevated bilirubin.
Results
A total of 610 adults with primary CAD were included in the study (mean [SD] age 67.9 [14.5] years, 65.4% female). The mean (SD) duration of follow-up was 48.1 (30.6) months; 90% of patients had ≥12 months of follow-up. At baseline (0-6 months prior to first mention of CAD), 47.6% of patients had elevated bilirubin levels and 63.1% had elevated lactate dehydrogenase (LDH) levels.
A high proportion of patients with CAD experienced severe or moderate anemia at baseline and in the 6 months post-baseline; this proportion tended to be lower, but still substantial, throughout the follow-up period (Table). Frequency of moderate/severe anemia or severe hemolysis events per patient year was also higher in the first 6 months: 5.70 (95% CI: 5.00, 6.49), compared with 2.92 (2.30, 3.71) and 2.43 (1.89, 3.11) events at months 19-24 and months 31-36, respectively.
The median number of CAD-related treatments per patient was high in all CAD patients at 6 months and remained high during the follow-up period (Table). The most common therapies used (excluding blood transfusion) were corticosteroids, antineoplastics and biologics. The mean number of blood transfusions per patient was higher in the severe anemia category at all follow-up intervals. The number of hospitalizations and emergency room visits were generally higher in patients with increased anemia severity; outpatient visits were high in all CAD patients and remained so over the study period (Table).
Conclusion
This observational cohort study followed a large sample of primary CAD patients with a 4-year mean follow-up. The results highlight the long-term substantial burden of CAD on patients and healthcare systems, which generally increased with higher severity of anemia. Three years after diagnosis, the number of moderate to severe anemia or hemolysis events remained high in CAD patients, despite off-label CAD management. The need for blood transfusions was still substantial in the severe anemic population 3 years after diagnosis. This longitudinal analysis illustrates the unmet medical needs in primary CAD.
Wilson:Sanofi: Current Employment, Current equity holder in publicly-traded company. Joly:Sanofi: Current Employment, Current equity holder in publicly-traded company. Miles:Aetion Inc.: Current Employment, Other: Employee of software company that received funding from Sanofi for the current study. Kuang:Aetion Inc.: Current Employment, Other: Employee of software company that received funding from Sanofi for the current study. Pham:Sanofi: Consultancy; Alexion: Other: Speaker.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal