

Background
Haploidentical allogeneic hematopoietic cell transplantation (haplo-HCT) with post-transplant cyclophosphamide (PTCy) has greatly expanded potential donor options for patients (pts) without a fully HLA-matched donor. However, an HLA-mismatched unrelated donor (UD) or cord blood transplantation (CBT) are valid options for pts who do not have an haploidentical-related or a fully HLA-matched donor. The incorporation of PTCy with mismatched UD allo-HCT is associated with reduced risk of non-relapse mortality (NRM) and graft-versus-host disease (GvHD) (Jorge et al., BBMT, 2018). No previous study has compared outcomes of these two graft sources in contemporary era. In this study, we compared the outcomes of CBT versus (vs) single antigen-mismatched (HLA 9/10) UD allo-HCT with post-transplant cyclophosphamide (PTCy) in pts with acute myeloid leukemia (AML).
Methods
Pts with AML who underwent a first CBT without PTCy (N=902) or allo-HCT from a 9/10 UD with PTCy (N=280) between 2010 to 2019 were selected from The European Society of Blood and Marrow Transplantation (EBMT) registry. We excluded pts who had ex vivo T cell depletion. The median pt age was comparable between CBT and UD cohort [51 years (y) vs. 52 y, p=0.09]. The recipients of CBT had a longer median follow up (47 vs. 19 months, p<0.01) compared to UD. The cytogenetic risk category was good in 68 (6%), intermediate in 514 (46%), poor in 184 (16%) and unknown in 416 (35%) pts. Pre-HCT disease status was first complete remission (CR1) in 701 (59%), CR2 in 279 (24%) and advanced (non-CR1/CR2) in 202 (17%) pts. Myeloablative conditioning (MAC) was used in 47% of the total pts and the use of MAC was comparable between the study cohorts (p=0.21). In vivo T cell depletion was used more frequently with CBT compared to UD (40% vs. 26%, p<0.01). A Cox regression multivariate (MV) analysis was performed for the whole population. A matched-pair analysis was carried out by propensity score based 1:1 matching of pts with known cytogenetic risk. Propensity score was based on pt age, gender, Karnofsky performance score, cytogenetic risk group, pre-HCT disease status and intensity of conditioning regimen.
Results
In the univariate analysis, day +180 incidence of grade II-IV acute GvHD was 36% vs. 32% (p=0.07) and grade III-IV acute GvHD was 15% vs. 11% (p=0.16) for CBT and UD cohorts, respectively. The 2-y incidence of total chronic GvHD was 26% vs. 32% (p=0.20) and extensive chronic GvHD was 12% vs. 12% (p=0.83), respectively. CBT was associated with higher incidence of graft failure (11% vs. 4%, p<0.01) and higher 2y NRM (30% vs. 16%, p<0.01) compared to UD. CBT resulted in lower leukemia free survival (LFS) (43% vs. 61%, p<0.01), overall survival (OS) (47% vs. 63%, p<0.01) and GvHD-free, relapse-free survival (GRFS) (34% vs. 47%, p<0.01). There was no difference in 2y relapse incidence (RI) between study cohorts (28% vs. 23%, p=0.24). There were more infection-related deaths in CBT compared to UD allo-HCT recipients (31% vs. 24% of total reported deaths). Among CBT recipients, 3 pts died from graft failure and 5 pts died from lymphoproliferative disorder.
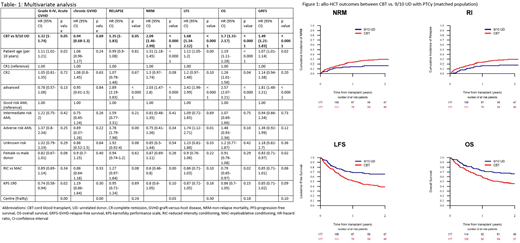
In the MV analysis (Table 1), CBT was associated with higher risk of grade II-IV acute GvHD [hazard ratio (HR)=1.32, 95% confidence interval (CI):1-1.74,p<0.05], NRM [HR=2.09, 95% CI:1.46-2.99, p<0.0001], and RI [HR=1.35, 95% CI: 1-1.83, p=0.05] which resulted in inferior LFS [HR=1.68, 95% CI:1.34-2.12,p<0.0001], OS [HR=1.7, 95% CI:1.33-2.17, p<0.0001] and GRFS [HR=1.49, 95% CI:1.21-1.83,p<0.0001] compared to UD. The chronic GvHD did not differ between the study cohorts [HR=0.94, 95% CI: 0.68-1.3, p=0.69]. Older age and advanced disease status were associated with poor OS. These results were confirmed in a matched-pair analysis, which compared 177 pairs of CBT vs. 9/10 UD allo-HCT pts. CBT was associated with higher 2y NRM (HR=1.96, p<0.01), RI (HR=2.01, p<0.01), and lower LFS (HR=1.98 p<0.01), OS (HR=1.82, p<0.01) and GRFS (HR=1.77, p<0.01) (Figure 1). Grade II-IV acute (HR=1.33, p=0.13) and total chronic (HR=1.02, p=0.93) GvHD rates were comparable between the cohorts.
Conclusions
In this large registry-based observational study, CBT was associated with inferior LFS, OS and GRFS due to higher NRM and RI compared to 9/10 UD allo-HCT with PTCy. In the absence of a fully matched or haplo donor, 9/10 UD allo-HCT with PTCy may be preferred over CBT in pts with AML. A prospective study is needed to validate our findings.
Dholaria:Poseida: Research Funding; Angiocrine: Research Funding; Takeda: Research Funding; J&J: Research Funding; bms: Research Funding. Labopin:Jazz Pharmaceuticals: Honoraria. Blaise:Jazz Pharmaceuticals: Honoraria. Chevallier:Incyte Corporation: Honoraria. Mohty:BMS: Consultancy, Honoraria, Research Funding, Speakers Bureau; Celgene: Consultancy, Honoraria, Research Funding, Speakers Bureau; Takeda: Consultancy, Honoraria, Research Funding, Speakers Bureau; Stemline: Consultancy, Honoraria, Research Funding, Speakers Bureau; GSK: Consultancy, Honoraria, Research Funding, Speakers Bureau; Jazz Pharmaceuticals: Consultancy, Honoraria, Research Funding, Speakers Bureau; Novartis: Consultancy, Honoraria, Research Funding, Speakers Bureau; Sanofi: Consultancy, Honoraria, Research Funding, Speakers Bureau; Janssen: Consultancy, Honoraria, Research Funding, Speakers Bureau; Amgen: Consultancy, Honoraria, Research Funding, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal