

Background Survival rates of childhood cancers have improved substantially over the past four decades. However, these improvements have been accompanied by substantial long-term morbidity and premature mortality. In this study, we analyzed trajectory groups that correlate with long-term mortality in childhood cancer survivors.
Methods The National Health Insurance Service (NHIS) database is a population-based cohort covering over 95% of the population across all regions of South Korea. We used the patient-level longitudinal NHIS database which included patients who first received a cancer code ([ICD 10: C]) under the age of 20 years from 2002-2017. The onset of cancer diagnosis was defined as the time of the earliest diagnosis in patients who were prescribed any treatment excluding surgery within one month after the initial diagnosis. Claims codes for chemotherapeutic agents, radiotherapy, and transplantation were designated and analyzed in the database. For trajectory analysis, the total numbers of claimed diagnostic codes per year were used as the input variable of the group-based trajectory method. The separate trajectories were identified using the Proc Traj procedure in SAS 9.4.
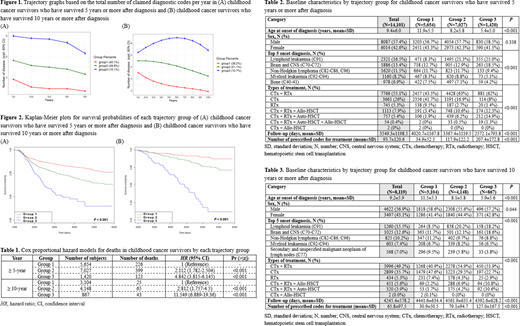
Results A total of 71,323 people were extracted from the NHIS database. After washing out previously diagnosed patients in 2002, 58,964 people remained from 2003-2017. We included 14,101 patients without records of any treatment for 3 years after the first diagnosis in the final analysis. Trajectory groups were generated in 14,101 and 8,119 patients who have survived more than 5 years and more than 10 years, respectively. Among the ≥ 5 years survivors, three groups were classified: Group 1 (N=5,654; 40.1%), Group 2 (N=7,027; 49.8%), and Group 3 (N=1,420, 10.1%) (Figure 1(A)). Likewise, three trajectory groups were identified in ≥ 10 years survivors: Group 1 (N=3,104; 38.2%), Group 2 (N=4,148; 51.1%), and Group 3 (N=867; 10.7%) (Figure 1(B)).
Notably, the risk of death was significantly different between each trajectory group according to Cox regression analysis after being corrected for age and sex (Table 1). In patients with a follow-up of 5 years or more, mortality risk was 4.84 times higher in Group 3 compared to Group 1 (P<0.001). Also, in patients with follow-up of 10 years or more, mortality risk was 11.55 times higher in Group 3 compared with Group 1 (P<0.001). In the survival graph from the timepoints of 5 or 10 years after diagnosis, there were significant differences in overall survival between each trajectory group of the two patient cohorts (P<0.001, Figure 2).
To identify characteristics associated with survival differences between trajectory groups, baseline characteristics at diagnosis and treatments were analyzed (Table 2, 3). There were significant differences in age at time of diagnosis in three trajectory groups: in both cohorts, age at diagnosis was significantly younger in Group 3 of the lowest survival rates than other groups. For initial diagnosis, there were increasing trends of Lymphoid leukemia and brain tumors in Group 3 of both cohorts. For types of treatment, the proportions of patients who received only chemotherapy or radiotherapy decreased from Group 1 to Group 3. However, the proportions of patients who received combined treatment with any stem cell transplantation increased from Group 1 to Group 3. The follow-up periods were significantly lower in Group 3, which corresponded to the survival probabilities. Whereas the numbers of prescribed codes for any treatment were significantly higher in Group 3, indicating that patients in Group 3 received more frequent and condensed treatments within shorter periods than those in Group 2, and this relationship was also seen between Group 2 and Group 1.
Conclusions This study is the first trajectory analysis conducted in childhood cancer survivors using population-based longitudinal data. In this study, unlike previous trajectory analyses based on characteristics at the time of diagnosis, trajectories were classified based on the burden of diagnosis during periods, which resulted in differences in long-term mortality, and then the differences in characteristics between each group were analyzed. Our findings indicate that that long-term mortality is related to age at diagnosis and concentration of treatment relative to total follow-up duration rather than the absolute duration or intensity of treatment.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal