

Introduction and objective. Despite a high complete remission (CR) rate obtained with frontline therapy most adults with T-ALL eventually relapse. Although promising therapies are emerging, salvage options for T-ALL are currently limited. Little is known about outcome of patients (pts) with relapsed T-ALL (R T-ALL) treated with contemporary MRD-oriented trials. Our goal was to analyze the outcome of pts with R T-ALL included in two successive MRD-oriented trials (ALL-AR-03 and ALL-HR-11) from the Spanish PETHEMA Group.
Methods. Retrospective study of R T-ALL adults diagnosed between 2003 and 2019 and included in the protocols ALL-AR-03 (NCT00853008) and ALL-HR-11 (NCT01540812). The clinical characteristics at baseline and at relapse, salvage therapies and outcomes (CR and OS) were analyzed and a study of prognostic factors for OS was performed.
Results
Forty-nine patients were identified (ALL-AR-03 [n=27], ALL-HR-11 [n=22]). Median age (range) at diagnosis was 29 (16-58) yrs, 38 males (78%), CNS involvement 6 (12%), mediastinal mass 30 (61%), WBC count 40.8 x109/L (0.6-351.0), early T-cell precursor 11 (23%), pre-T 8 (16%), cortical 16 (33%), mature 9 (18%), T unspecified 5 (10%). Post-induction-1 MRD level ≥0.1%: 14/42 (33%), ≥0.01%: 17/39 (44%). Nine pts (18%) required 2nd induction therapy (resistant disease after induction-1 [n=5], MRD≥0.1% after induction-1 [n=4]). Allogeneic HSCT in CR1: 8 pts. Interval CR1-relapse: 11.2 [0.1-36.7] months. Relapse was located in BM (n=20, 41%), BM+extramedullary (n=16, 33%) and extramedullary (n=13, 26%). CNS at relapse was involved in 18 pts (37%, isolated in 8 cases).
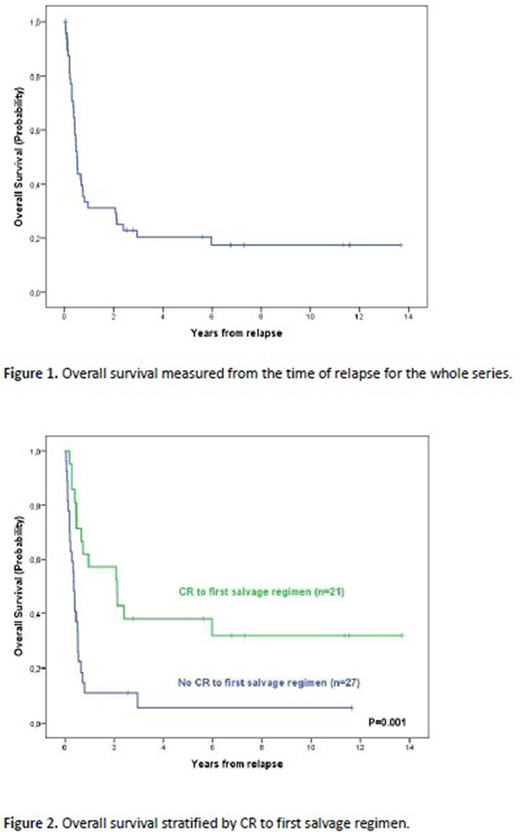
Median number of rescue lineages was 2 (range 1-5). The most frequent first salvage schedules were FLAG-Ida (n=24, 49%), HyperCVAD (n=8, 16%) and nelarabine (n=4, 8%) (other schedules in 13 pts). Second CR was attained in 21/48 pts (44%). The patients with poor morphologic and/or poor MRD response after Induction-1 in first line therapy (n=9) did not respond to first salvage therapy (0/9 vs. 21/39, p=0.003). AlloHSCT was performed in 19 pts (15 in CR2) (HLA-identical sibling: 9, URD: 9, haploidentical: 1, myeloablative conditioning: 16). Thirty-nine pts died (progression: 27, toxicity of rescue regimens: 7, TRM: 5) and 9/10 alive patients were submitted to HSCT (the remaining is on rescue therapy). Median OS (95%CI) was 6.1 (4.9-7.2) months, 5yr OS probability 21% (9%-33%) (Figure 1). By multivariable analysis, only the CR after first salvage regimen emerged as favorable prognostic factor for OS (HR 3.110, 95%CI: 1.579-6.124) (Figure 2).
Conclusion. This study shows poor outcome of adults with R T-ALL, with CR to first salvage therapy of 44% and a median OS of 6 months. Poor early response to first line therapy correlated with poor response to salvage-1. The only independent predictor for better survival was CR to first salvage regimen. This study highlights the unmet need for novel effective therapies for T-ALL.
Supported in part by grant 2017 SGR288 (GRC) Generalitat de Catalunya and "La Caixa" Foundation; ISCIII (PI19/01828), co-funded by ERDF/ESF, "A way to make Europe"/"Investing in your future".
Ribera:Pfizer, Amgen, Ariad, Novartis: Consultancy, Speakers Bureau; Pfizer, Amgen: Research Funding. Barba:Amgen, Celgene, Gilead, Jazz Pharmaceuticals, Novartis, Pfizer, Shire: Consultancy; Amgen, Celgene, Novartis, Pfizer: Speakers Bureau. Tormo:Celgene: Honoraria, Membership on an entity's Board of Directors or advisory committees; Pfizer: Honoraria; Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees; Janssen: Honoraria; MSD: Honoraria; Daiichi Sankyo: Honoraria; Servier: Honoraria; Roche: Membership on an entity's Board of Directors or advisory committees; Astellas: Membership on an entity's Board of Directors or advisory committees. Sanchez:Abbvie: Other: travel grants; Amgem: Other: travel grants; Janssen: Other: travel grants; Celgene: Other: travel grants; Roche: Other: travel grants. Giménez Conca:AbbVie: Honoraria, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal