

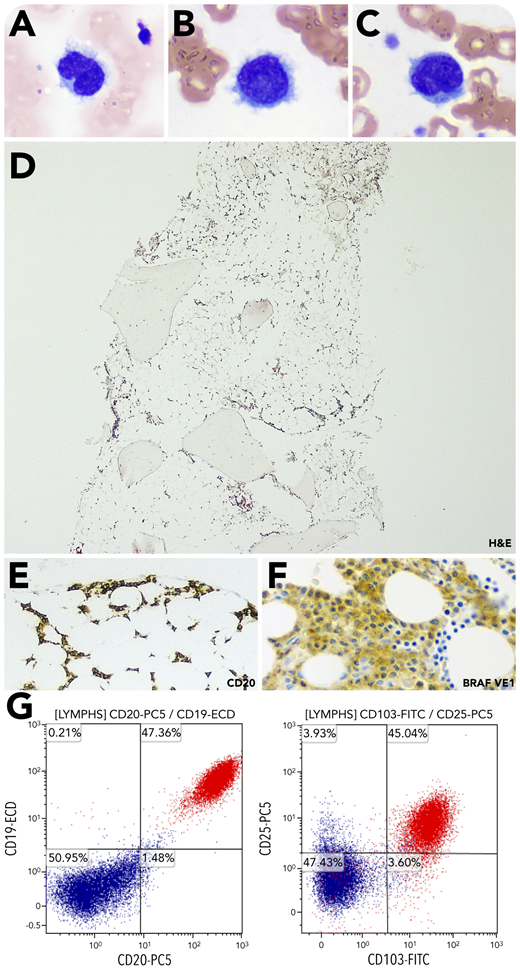
A 56-year-old man underwent a bone marrow (BM) biopsy for leukopenia of several years. Hemogram revealed a low white blood cell count of 1.8 × 109/L (reference, 4.5-11 × 109/L; differential: 47% neutrophils, 46% lymphocytes, 4% monocytes) and thrombocytopenia (platelets = 100 × 109/L; reference, 150-450 × 109/L). Hemoglobin was within normal limits. The BM aspirate smear disclosed marrow particles with atypical lymphocytes characterized by reniform nuclei, reticular chromatin, absent nucleoli, and circumferential cytoplasmic projections (panels A-C, original magnification ×1000, Wright-Giemsa stain). The core biopsy revealed a markedly hypocellular marrow, with ∼10% cellularity (panel D, original magnification ×40, hematoxylin and eosin stain), which was composed predominantly of small lymphocytes positive for CD20 and BRAFVE1 (a mouse monoclonal antibody against BRAF V600E mutant) (panels E-F, original magnification ×500, CD20 and BRAFVE1). Flow cytometry identified λ-restricted B cells expressing CD20 (bright), CD22 (bright), CD103, and CD25 (panel G). Molecular testing confirmed BRAFV600E mutation. Radiographic studies did not show splenomegaly or lymphadenopathy.
The cytologic, immunophenotypic, and molecular findings are characteristic and diagnostic of hairy cell leukemia (HCL). BM hypocellularity, mimicking aplastic anemia, and lack of splenomegaly are uncommon in HCL and may be confounding features in the diagnostic work-up. HCL should be a consideration when faced with a hypocellular BM. In these atypical cases, complete assessment by immunohistochemistry and flow cytometry, as well as thorough review of cytomorphology, is essential in arriving at the diagnosis.
A 56-year-old man underwent a bone marrow (BM) biopsy for leukopenia of several years. Hemogram revealed a low white blood cell count of 1.8 × 109/L (reference, 4.5-11 × 109/L; differential: 47% neutrophils, 46% lymphocytes, 4% monocytes) and thrombocytopenia (platelets = 100 × 109/L; reference, 150-450 × 109/L). Hemoglobin was within normal limits. The BM aspirate smear disclosed marrow particles with atypical lymphocytes characterized by reniform nuclei, reticular chromatin, absent nucleoli, and circumferential cytoplasmic projections (panels A-C, original magnification ×1000, Wright-Giemsa stain). The core biopsy revealed a markedly hypocellular marrow, with ∼10% cellularity (panel D, original magnification ×40, hematoxylin and eosin stain), which was composed predominantly of small lymphocytes positive for CD20 and BRAFVE1 (a mouse monoclonal antibody against BRAF V600E mutant) (panels E-F, original magnification ×500, CD20 and BRAFVE1). Flow cytometry identified λ-restricted B cells expressing CD20 (bright), CD22 (bright), CD103, and CD25 (panel G). Molecular testing confirmed BRAFV600E mutation. Radiographic studies did not show splenomegaly or lymphadenopathy.
The cytologic, immunophenotypic, and molecular findings are characteristic and diagnostic of hairy cell leukemia (HCL). BM hypocellularity, mimicking aplastic anemia, and lack of splenomegaly are uncommon in HCL and may be confounding features in the diagnostic work-up. HCL should be a consideration when faced with a hypocellular BM. In these atypical cases, complete assessment by immunohistochemistry and flow cytometry, as well as thorough review of cytomorphology, is essential in arriving at the diagnosis.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal