

Key Points
Anticoagulant therapy was associated with a high rate of splanchnic vein recanalization and a low rate of thrombosis progression.
Major bleeding risk and overall mortality of patients with splanchnic vein thrombosis were reduced by anticoagulant therapy.

Abstract
Treatment of splanchnic vein thrombosis (SVT) is challenging, and evidence to guide therapeutic decisions remains scarce. The objective of this systematic review and meta-analysis was to determine the efficacy and safety of anticoagulant therapy for SVT. MEDLINE, EMBASE, and clinicaltrials.gov were searched from inception through December 2019, without language restrictions, to include observational studies and randomized controlled trials reporting radiological or clinical outcomes in patients with SVT. Pooled proportions and risk ratios (RRs) with 95% confidence intervals (CIs) were calculated in a random-effects model. Of 4312 records identified by the search, 97 studies including 7969 patients were analyzed. In patients receiving anticoagulation, the rates of SVT recanalization, SVT progression, recurrent venous thromboembolism (VTE), major bleeding, and overall mortality were 58% (95% CI, 51-64), 5% (95% CI, 3-7), 11% (95% CI, 8-15), 9% (95% CI, 7-12), and 11% (95% CI, 9-14), respectively. The corresponding values in patients without anticoagulation were 22% (95% CI, 15-31), 15% (95% CI, 8-27), 14% (95% CI, 9-21), 16% (95% CI, 13-20), and 25% (95% CI, 20-31). Compared with no treatment, anticoagulant therapy obtained higher recanalization (RR, 2.39; 95% CI, 1.66-3.44) and lower thrombosis progression (RR, 0.24; 95% CI, 0.13-0.42), major bleeding (RR, 0.73; 95% CI, 0.58-0.92), and overall mortality (RR, 0.45; 95% CI, 0.33-0.60). These results demonstrate that anticoagulant therapy improves SVT recanalization and reduces the risk of thrombosis progression without increasing major bleeding. The incidence of recurrent VTE remained substantial in patients receiving anticoagulation, as well. Effects were consistent across the different subgroups of patients. This trial was registered on the PROPERO database at (https://www.crd.york.ac.uk/prospero//display_record.php?ID=CRD42019127870) as #CRD42019127870.
Introduction
Splanchnic vein thrombosis (SVT) includes portal, mesenteric, or splenic vein thrombosis and Budd-Chiari syndrome (BCS).1 While the incidence of deep vein thrombosis of the limbs and pulmonary embolism is ∼70-270 per 100 000 patients, the incidence of SVT is at least 25 times lower, with the most and least common types being represented by portal vein thrombosis (PVT) and BCS, respectively.2,3 Common risk factors for SVT include liver cirrhosis, solid cancer, and myeloproliferative neoplasms. SVT may also be related to transient risk factors (eg, surgery, abdominal inflammation or infection, hormonal replacement therapy, or pregnancy) and is defined as unprovoked in 15% to 27% of cases.3-5 In approximately one-third of patients, SVT is incidentally detected during abdominal imaging performed for other reasons.4-8
Treatment of SVT is challenging and requires careful evaluation of risk factors for SVT progression, recurrence of VTE, and bleeding. The latter may be substantial, in particular in patients with underlying cirrhosis and/or cancer, because of frequent comorbidities such as thrombocytopenia and gastroesophageal varices.9 Several observational studies that evaluated the effects of anticoagulant therapy on the rates of recanalization and progression, recurrent VTE, and bleeding in patients with SVT reported conflicting findings.1,10 As a result of the large clinical variability of SVT and the limited evidence available, current treatment recommendations vary widely across clinical practice guidelines, and the decisions regarding which patients should be treated and the type, dose, or duration of anticoagulant therapy are often made empirically.1,9-13 A better understanding of the average risk of clinically relevant outcomes in patients with SVT may help physicians in daily clinical practice and inform the design of future studies.
The objective of this systematic review and meta-analysis was therefore to evaluate radiological and clinical outcomes in patients with SVT receiving or not receiving anticoagulant therapy.
Methods
This study-level systematic review and meta-analysis was performed according to Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines.14
Databases search and study selection
MEDLINE and EMBASE were searched from inception through December 2019 for observational studies and randomized controlled trials (RCTs) involving patients with SVT. Furthermore, we searched clincaltrial.gov for ongoing or completed studies and screened references of the relevant studies. No language restrictions were applied. The complete search strategy is given in supplemental Table 1, available on the Blood Web site.
Two of the authors independently reviewed titles and abstracts identified from the databases searched, to select studies that met the following inclusion criteria: (1) diagnosis of SVT; (2) observational study or RCT including ≥10 patients; (3) availability of radiological (recanalization or progression of SVT) or clinical (recurrent VTE, major bleeding, and overall mortality) outcomes; and (4) anticoagulant treatment with low-molecular-weight heparin (LMWH), unfractionated heparin, fondaparinux, vitamin K antagonists (VKAs), direct oral anticoagulants (DOACs), or no anticoagulant therapy. Exclusion criteria were any of the following: (1) study design different from those specified in the inclusion criteria; (2) inclusion of <10 patients; and (3) anticoagulant therapy different from those specified in the inclusion criteria.
Any disagreement was resolved through discussion or the opinion of a third review author.
Data extraction and quality assessment
Two review authors independently extracted data from the included studies. A consensus between the 2 review authors or a discussion with a third review author resolved any disagreement.
The following data were extracted: methodological quality; study design; patient characteristics (eg, age, sex); site, extension, and stage of SVT; risk factors for SVT; type and duration of anticoagulant treatment; and radiological (recanalization or progression of SVT) or clinical (recurrent VTE, major bleeding, and overall mortality) outcomes. Published supplemental materials were searched for data of interest, and corresponding authors were contacted in case of missing information.
The risk of bias of the included studies and the summary of the risk of bias were evaluated using the ROBINS-I tool for observational studies and the Cochrane tool for RCTs.15,16
Study outcomes
The radiological outcomes included any grade of recanalization (partial or complete) and progression of SVT at follow-up imaging. The clinical outcomes were recurrent VTE (deep vein thrombosis of the lower or upper extremities, pulmonary embolism, or recurrent SVT); major bleeding, as defined by study authors or interpreted as major by the review authors; and overall mortality.
Statistical analysis
The logit-transformed proportion and corresponding sampling variances were calculated. Pooled proportions and risk ratios (RRs) with corresponding 95% confidence intervals (CIs) were calculated in a random-effects model. Heterogeneity among the included studies was evaluated by visual inspection of forest plots and by the DerSimonian-Laird estimator and was defined as low, moderate, or high for I2 values of 25%, 50%, and 75%, respectively.17 In cases of heterogeneity, we performed a random-effect subgroup analysis to explore the effects of the following variables: (1) site of thrombosis (portal, mesenteric, splenic, BCS, and multiple veins); (2) stage of thrombosis (acute or recent, if ≤6 months; chronic, if >6 months; mixed; and not reported); (3) clinical presentation (symptomatic, incidental, mixed, and not reported); (4) risk factor (transient, persistent risk factor or unprovoked SVT, or multiple risk factors); (5) type of therapy (parenteral, oral, or mixed); (6) duration of therapy (≤6 months, >6 months, and not reported); (7) study design (retrospective, prospective, ambispective, or RCT). We decided a priori to include a study in one of the subgroups according to patient or SVT characteristics if the latter were present in more than 75% of patients included in that study. A mixed-effects model with restricted maximum-likelihood estimator was performed fitting the specified variables as moderators, whenever available.
A sensitivity analysis was planned to evaluate the effects of anticoagulant therapy in patients with different underlying risk factors (eg, liver cirrhosis, solid cancer, or myeloproliferative neoplasms) and to evaluate the effect of different types of anticoagulant therapy (LMWH alone, LMWH followed by VKAs, VKAs alone, and DOACs) on radiological and clinical outcomes.
The presence of publication bias was assessed in patients receiving anticoagulation by funnel plot of logit-transformed proportion vs standard error. Funnel plot symmetry was tested by performing the Egger test. If the test confirmed asymmetry, we used Duval and Tweedie’s trim-and-fill procedure to compute an unbiased estimate of the effect size.
Statistical analyses were performed with R studio version 1.2.5001, “meta,” “metafor,” and “forestplot” packages.18 Summary forest plots were prepared with STATA/SE v.12 (StataCorp LP, College Station, TX). P < .05 indicated statistically significant differences.
Results
Figure 1 shows the PRISMA flow diagram. A total of 4309 records were identified from the literature search. Screening of the clinicaltrials.gov database found 3 additional ongoing studies that had no results available. After 621 duplicates were removed, 3544 records were excluded by title and abstract screening. Full-text evaluation excluded 50 studies. Finally, 97 studies including 7969 patients were considered in the analysis (the full list of included studies is available in the supplemental Table 2).
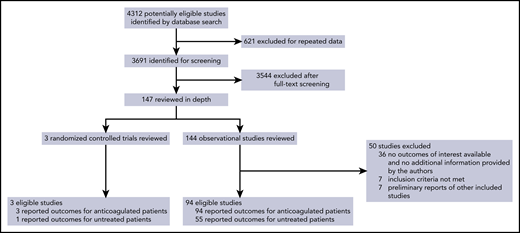
The interreviewer agreement was excellent, with a κ statistic of 0.88.
Characteristics of included studies
Three studies were RCTs, and 94 were observational with a prospective (n = 20), retrospective (n = 71), or ambispective (n = 3) design. Sample sizes ranged from 10 to 832 patients. At least 1 of the radiological outcomes was reported by 56 studies (57.7%) and at least 1 clinical outcome by 91 studies (93.8%). Median treatment duration was 8.4 months (range, 0.4-108 months; 36 studies), and median follow-up was 28.6 months (range, 6-144 months; 62 studies). The main characteristics of the included studies are reported in supplemental Table 2.
Risk of bias across domains was low, moderate, serious, and critical in 0%, 13.8% (n = 13), 70.2% (n = 66), and 16.0% (n = 15) of the observational studies, respectively. The risk of bias was high for blinding of participants and personnel in 2 RCTs and for incomplete outcome data in 1 trial. The risk-of-bias summary is shown in supplemental Figure 1 and supplemental Table 3 for observational studies and in supplemental Figure 2 for RCTs.
Characteristics of the overall study population
The main characteristics of the overall population are reported in Table 1. The mean age was 49.2 ± 10.3 years, and 4404 (55.8%) of the patients were men. Patients with portal, mesenteric, or splenic SVT, BCS, and multiple sites of SVT were included in 63 studies (3365 of 6192 patients; 54.3%), 35 studies (1015 of 4271 patients; 23.8%), 18 studies (452 of 3570 patients; 12.7%), 25 studies (1153 of 3624 patients; 31.8%), and 64 studies (2297 of 5937 patients; 38.7%), respectively. A total of 57 studies specified whether SVT was acute or recent (2607 of 3424 patients; 76.1%) or chronic (770 of 3424 patients; 22.5%). The most common risk factors for SVT were liver cirrhosis (2578 of 5518 patients; 46.7%; 51 studies), followed by myeloproliferative neoplasm (1429 of 4598 patients; 31.1%; 43 studies) and solid cancer (1108 of 4787 patients; 23.1%; 42 studies). SVT was unprovoked in 25.1% of patients (770 of 3070 patients; 35 studies).
Characteristics of study population (n = 7969) from 97 studies
| Data | Studies reporting the variable, n | |
|---|---|---|
| Patients characteristics | ||
| Age, mean (SD), years | 49.2 ± 10.3 | 91 |
| Male sex, n/N (%) | 4404/7886 (55.8) | 95 |
| Site of SVT | ||
| Portal vein thrombosis, n/N (%) | 3365/6192 (54.3) | 63 |
| Mesenteric vein thrombosis, n/N (%) | 1015/4271 (23.8) | 35 |
| Splenic vein thrombosis, n/N (%) | 452/3570 (12.7) | 18 |
| Budd-Chiari syndrome, n/N (%) | 1153/3624 (31.8) | 25 |
| Multiple sites thrombosis, n/N (%) | 2297/5937 (38.7) | 64 |
| Not reported, n/N (%) | 55/220 (25.0) | 6 |
| Vein involvement | ||
| Partial, n/N (%) | 521/853 (61.1) | 20 |
| Complete, n/N (%) | 306/853 (35.9) | 20 |
| Not reported, n/N (%) | 26/853 (3.0) | 20 |
| Stage of thrombosis | ||
| Acute/recent, n/N (%) | 2607/3424 (76.1) | 57 |
| Chronic, n/N (%) | 770/3424 (22.5) | 57 |
| Not reported, n/N (%) | 47/3424 (1.4) | 57 |
| Risk factors | ||
| Liver cirrhosis, n/N (%) | 2578/5518 (46.7) | 51 |
| Myeloproliferative neoplasm, n/N (%) | 1429/4598 (31.1) | 43 |
| Unprovoked, n/N (%) | 770/3070 (25.1) | 35 |
| Solid cancer, n/N (%) | 1108/4787 (23.1) | 42 |
| Surgery, n/N (%) | 642/3762 (17.1) | 44 |
| Abdominal inflammation/infection, n/N (%) | 726/4346 (16.7) | 41 |
| Hormonal replacement therapy, n/N (%) | 297/3250 (9.1) | 31 |
| Thrombophilia | ||
| JAK2 V617F, n positive/N tested (%) | 148/802 (18.5) | 9 |
| Antiphospholipid syndrome, n positive/N tested (%) | 135/1064 (12.7) | 20 |
| Factor V Leiden mutation, n positive/N tested (%) | 224/1938 (11.6) | 28 |
| Protein C and/or S deficiency, n positive/N tested (%) | 125/1085 (11.5) | 21 |
| Prothrombin G2021A mutation, n positive/N tested (%) | 112/1257 (8.9) | 15 |
| Antithrombin-III deficiency, n positive/N tested (%) | 30/904 (3.3) | 13 |
| Diagnosis of SVT | ||
| Computed tomography, n/N (%) | 3418/4973 (68.7) | 56 |
| Doppler ultrasonography, n/N (%) | 1794/4645 (38.6) | 49 |
| Angiography, n/N (%) | 265/2627 (10.1) | 16 |
| Magnetic resonance imaging, n/N (%) | 297/3633 (8.2) | 24 |
| Perioperative, n/N (%) | 153/2378 (6.4) | 13 |
| Follow-up imaging | ||
| Ultrasonography, n/N (%) | 484/494 (98.0) | 13 |
| Computed tomography, n/N (%) | 507/678 (74.8) | 16 |
| Median follow-up, mo | 28.6 (6 to 144) | 62 |
| Parenteral anticoagulation | ||
| LMWH, n/N (%) | 1038/2365 (43.9) | 24 |
| LMWH or UFH, n/N (%) | 383/1785 (21.5) | 13 |
| Fondaparinux, n/N (%) | 26/703 (3.7) | 2 |
| Oral anticoagulation | ||
| LMWH→VKAs, n/N (%) | 1320/2672 (49.4) | 40 |
| VKAs, n/N (%) | 1892/5170 (36.6) | 39 |
| DOACs, n/N (%) | 142/1125 (12.6) | 9 |
| Antiplatelet therapy | 189/2569 (7.4) | 15 |
| Mixed strategies, n/N (%) | 505/1817 (27.8) | 22 |
| No anticoagulation, n/N (%) | 1424/5416 (26.3) | 66 |
| Systemic or catheter directed thrombolysis, n/N (%) | 207/2477 (8.4) | 25 |
| Median treatment duration, months | 8.4 (0.4 to 108) | 36 |
| Other therapeutic procedures | ||
| Thrombectomy/stenting, n/N (%) | 176/1656 (10.6) | 16 |
| TIPS, n/N (%) | 482/2960 (16.3) | 26 |
| Liver transplantation, n/N (%) | 191/1634 (11.7) | 20 |
| Surgery, n/N (%) | 154/1259 (12.2) | 20 |
| Data | Studies reporting the variable, n | |
|---|---|---|
| Patients characteristics | ||
| Age, mean (SD), years | 49.2 ± 10.3 | 91 |
| Male sex, n/N (%) | 4404/7886 (55.8) | 95 |
| Site of SVT | ||
| Portal vein thrombosis, n/N (%) | 3365/6192 (54.3) | 63 |
| Mesenteric vein thrombosis, n/N (%) | 1015/4271 (23.8) | 35 |
| Splenic vein thrombosis, n/N (%) | 452/3570 (12.7) | 18 |
| Budd-Chiari syndrome, n/N (%) | 1153/3624 (31.8) | 25 |
| Multiple sites thrombosis, n/N (%) | 2297/5937 (38.7) | 64 |
| Not reported, n/N (%) | 55/220 (25.0) | 6 |
| Vein involvement | ||
| Partial, n/N (%) | 521/853 (61.1) | 20 |
| Complete, n/N (%) | 306/853 (35.9) | 20 |
| Not reported, n/N (%) | 26/853 (3.0) | 20 |
| Stage of thrombosis | ||
| Acute/recent, n/N (%) | 2607/3424 (76.1) | 57 |
| Chronic, n/N (%) | 770/3424 (22.5) | 57 |
| Not reported, n/N (%) | 47/3424 (1.4) | 57 |
| Risk factors | ||
| Liver cirrhosis, n/N (%) | 2578/5518 (46.7) | 51 |
| Myeloproliferative neoplasm, n/N (%) | 1429/4598 (31.1) | 43 |
| Unprovoked, n/N (%) | 770/3070 (25.1) | 35 |
| Solid cancer, n/N (%) | 1108/4787 (23.1) | 42 |
| Surgery, n/N (%) | 642/3762 (17.1) | 44 |
| Abdominal inflammation/infection, n/N (%) | 726/4346 (16.7) | 41 |
| Hormonal replacement therapy, n/N (%) | 297/3250 (9.1) | 31 |
| Thrombophilia | ||
| JAK2 V617F, n positive/N tested (%) | 148/802 (18.5) | 9 |
| Antiphospholipid syndrome, n positive/N tested (%) | 135/1064 (12.7) | 20 |
| Factor V Leiden mutation, n positive/N tested (%) | 224/1938 (11.6) | 28 |
| Protein C and/or S deficiency, n positive/N tested (%) | 125/1085 (11.5) | 21 |
| Prothrombin G2021A mutation, n positive/N tested (%) | 112/1257 (8.9) | 15 |
| Antithrombin-III deficiency, n positive/N tested (%) | 30/904 (3.3) | 13 |
| Diagnosis of SVT | ||
| Computed tomography, n/N (%) | 3418/4973 (68.7) | 56 |
| Doppler ultrasonography, n/N (%) | 1794/4645 (38.6) | 49 |
| Angiography, n/N (%) | 265/2627 (10.1) | 16 |
| Magnetic resonance imaging, n/N (%) | 297/3633 (8.2) | 24 |
| Perioperative, n/N (%) | 153/2378 (6.4) | 13 |
| Follow-up imaging | ||
| Ultrasonography, n/N (%) | 484/494 (98.0) | 13 |
| Computed tomography, n/N (%) | 507/678 (74.8) | 16 |
| Median follow-up, mo | 28.6 (6 to 144) | 62 |
| Parenteral anticoagulation | ||
| LMWH, n/N (%) | 1038/2365 (43.9) | 24 |
| LMWH or UFH, n/N (%) | 383/1785 (21.5) | 13 |
| Fondaparinux, n/N (%) | 26/703 (3.7) | 2 |
| Oral anticoagulation | ||
| LMWH→VKAs, n/N (%) | 1320/2672 (49.4) | 40 |
| VKAs, n/N (%) | 1892/5170 (36.6) | 39 |
| DOACs, n/N (%) | 142/1125 (12.6) | 9 |
| Antiplatelet therapy | 189/2569 (7.4) | 15 |
| Mixed strategies, n/N (%) | 505/1817 (27.8) | 22 |
| No anticoagulation, n/N (%) | 1424/5416 (26.3) | 66 |
| Systemic or catheter directed thrombolysis, n/N (%) | 207/2477 (8.4) | 25 |
| Median treatment duration, months | 8.4 (0.4 to 108) | 36 |
| Other therapeutic procedures | ||
| Thrombectomy/stenting, n/N (%) | 176/1656 (10.6) | 16 |
| TIPS, n/N (%) | 482/2960 (16.3) | 26 |
| Liver transplantation, n/N (%) | 191/1634 (11.7) | 20 |
| Surgery, n/N (%) | 154/1259 (12.2) | 20 |
TIPS, transjugular intrahepatic portosystemic shunt; UFH, unfractionated heparin.
The most frequent types of anticoagulant treatment were LMWH followed by VKAs (1320 of 2672 patients; 49.4%; 40 studies), LMWH alone (1038 of 2365 patients; 43.9%; 24 studies), and VKAs alone (1892 of 5170 patients; 36.6%; 39 studies). DOACs were used in 9 studies (142 of 1125 patients; 12.6%), either alone (96 of 142 patients; 67.6%; 3 studies) or in combination with another treatment (46 of 142 patients; 32.4%; 6 studies). Anticoagulant treatment was withheld in 26.3% of the patients (1424 of 5416; 66 studies). In addition to anticoagulant treatment, the use of systemic or catheter-directed thrombolysis was reported in 25 studies (207 of 2477 patients; 8.4%).
Radiological and clinical outcomes
Figure 2 and supplemental Figures 3-12 show the radiological and clinical outcomes in patients who received anticoagulation. In this group, 56 studies reported at least 1 radiological outcome, and 91 studies reported at least 1 clinical outcome. The rate of partial or complete recanalization was 58% (95% CI, 51-64; I2, 82%; 1017 of 1771 patients; 55 studies), the rate of progression of SVT was 5% (95% CI, 3-7; I2, 40%; 52 of 1416 patients; 47 studies), and the rate of recurrent VTE was 11% (95% CI, 8-15; I2, 81%; 266 of 3123 patients; 40 studies). Information on the type of recurrent VTE in patients who received anticoagulation were available for 127 patients (47.7%; 17 studies), of whom 80 had recurrent SVT; 19, stent or transjugular intrahepatic portosystemic shunt thrombosis; 19, deep vein thrombosis; 7, pulmonary embolism with or without deep vein thrombosis; and 2, cerebral vein thrombosis. Major bleeding occurred in 9% (95% CI, 7-12; I2, 85%; 491 of 4413 patients; 62 studies) and overall mortality in 11% (95% CI, 9-14; I2, 74%; 537 of 4501 patients; 76 studies).

Radiological and clinical outcomes in patients who received anticoagulant therapy.
Radiological and clinical outcomes in patients who received anticoagulant therapy.
Because of the limited availability of data, we performed a sensitivity analysis only on the subgroup of patients with liver cirrhosis. Results were similar to those for the overall population in terms of SVT recanalization (68%; 95% CI, 62-74), SVT progression (6%; 95% CI, 4-9), recurrent VTE (10%; 95% CI, 4-22), major bleeding (6%; 95% CI, 4-10), and overall mortality (9%; 95% CI, 6-14).
The rates of SVT recanalization seemed to vary across different types of anticoagulant treatment (P = .02), but was slightly higher with DOACs and LMWH (supplemental Figure 13). Conversely, the rates of thrombosis progression, recurrent VTE, major bleeding, and overall mortality were similar (supplemental Figures 14-17).
In patients receiving anticoagulation, there was evidence of publication bias for progression of SVT, major bleeding, and overall mortality (supplemental Figure 18).
Duval and Tweedie’s trim-and-fill procedure suggested significant variation in the effect size of anticoagulant treatment of progression of SVT, major bleeding, and overall mortality (supplemental Figure 19).
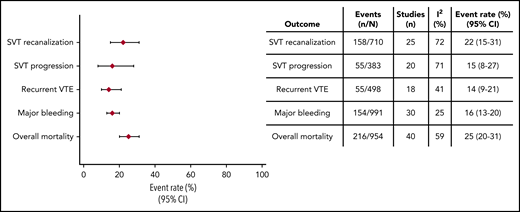
The outcome data for patients who did not receive anticoagulant treatment were available from 56 studies (Figure 3; supplemental Figures 20-24). The rate of partial or complete recanalization was 22% (95% CI, 15-31; I2, 72%; 158 of 710 patients; 25 studies). Progression of SVT occurred in 15% (95% CI, 8-27; I2, 71%; 55 of 383 patients; 20 studies), recurrent VTE in 14% (95% CI, 9-21; I2, 41%; 55 of 498 patients; 18 studies), major bleeding in 16% (95% CI, 13-20; I2, 25%, 154 of 991 patients; 30 studies), and overall mortality in 25% (95% CI, 20-31; I2, 59%; 216 of 954 patients; 40 studies). Information on the type of recurrent VTE in patients who remained untreated was available for 14 patients (25.9%; 2 studies) of whom 11 had recurrent SVT, 2 had transjugular intrahepatic portosystemic shunt thrombosis, and 1 had deep vein thrombosis.
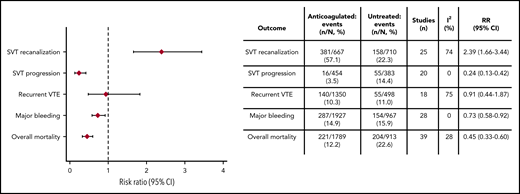
Fifty-five observational studies and 1 RCT included patients receiving anticoagulant treatment of SVT and untreated patients (Figure 4; supplemental Figures 25-29). The use of anticoagulant therapy was associated with higher recanalization (RR, 2.39; 95% CI, 1.66-3.44; I2, 74%; 25 studies) and lower progression of thrombosis (RR, 0.24; 95% CI, 0.13-0.42; I2, 0%; 20 studies), major bleeding (RR, 0.73; 95% CI, 0.58-0.92; I2, 0%; 28 studies), and overall mortality (RR, 0.45; 95% CI, 0.33-0.60; I2, 28%; 39 studies) compared with no treatment. The incidence of recurrent VTE was similar between the 2 groups (RR, 0.91; 95% CI, 0.44-1.87; I2, 75%; 18 studies).
Additional analyses in patients receiving anticoagulant therapy
The heterogeneity for the effects of anticoagulant treatment on radiological and clinical outcomes varied from low to high between studies and within each category of the subgroups evaluated (supplemental Figures 3-7; supplemental Table 4). The variables included in subgroup analysis (site or stage of SVT, clinical presentation, risk factor, type and duration of anticoagulant therapy, and study design) explained only a very small part of the interstudy heterogeneity (supplemental Table 4). Residual interstudy heterogeneity was low for progression of SVT, moderate for overall mortality, and high for SVT recanalization, recurrent VTE, and major bleeding (supplemental Table 4).
Because of information that was missing in the included studies, the type of risk factor (transient vs persistent risk factor–related or unprovoked SVT vs multiple risk factors), type of therapy (parenteral vs oral), and site of SVT (portal vs mesenteric veins vs BCS vs multiple veins) were fitted as moderators in mixed-effect models. The amount of heterogeneity explained by the model was 26.3% for recanalization of SVT, 16.6% for major bleeding, 13.0% for recurrent VTE, 0.8% for progression of SVT, and 0% for overall mortality. The test for residual heterogeneity was significant for all outcomes, indicating that other moderators that were not included in the model influenced interstudy heterogeneity (data available upon request). However, a higher rate of recanalization was found for isolated mesenteric vein thrombosis (RR, 14.1; 95% CI, 1.1-189.7) and for SVT that was unprovoked or associated with persistent thrombotic risk factors (RR, 4.2; 95% CI, 1.3-14.0).
Discussion
The results of this systematic review and meta-analysis show that vein recanalization was achieved in more than half of patients receiving anticoagulation, with relatively low rates of thrombosis progression. The risk of recurrent VTE remained substantial despite treatment, and major bleeding occurred in ∼10% of patients. The rate of vein recanalization was higher and progression of thrombosis was lower in patients who received therapy than in those who did not.
The estimation of the rates of relevant outcomes from a large population of patients with SVT may help in developing future studies and also in guiding the use of anticoagulant treatment of these patients.
The recanalization and progression of SVT have important prognostic implications, given their relationship with deterioration of hepatic function and risk of bleeding. SVT may lead to hypertension in the splanchnic circulation and the development of portosystemic collaterals, which increase the risk of gastrointestinal bleeding.19-21 Data for the effects of anticoagulant treatment on radiological outcomes varied broadly across the studies, ranging from 5.2% to 100% for recanalization and from 0% to 30.0% for SVT progression.22-27 We found that anticoagulant treatment may significantly improve radiological outcomes. However, there was high interstudy heterogeneity, which was explained only in part by the variables considered. Patients with SVT associated with persistent thrombotic risk factors and unprovoked SVT or isolated involvement of the mesenteric vein seemed to derive the greatest benefit in terms of vein recanalization. These findings should be interpreted very cautiously, because they may be influenced by unmeasured confounders such as duration of anticoagulation or use of additional treatments (eg, thrombolysis).
However, the rates of recurrent VTE were not negligible in patients who received anticoagulant treatment and were similar to the rates observed in untreated patients. This lack of benefit in the main clinical efficacy outcome may raise questions regarding the need for anticoagulation, although the sizeable variability in patient characteristics and, most of all, differences in anticoagulant regimens and treatment durations do not allow for any firm conclusion.
Conversely, a statistically significant reduction in the other 2 clinical outcomes considered, major bleeding and overall mortality, was found in patients who received anticoagulation. This result is relevant because patients with SVT often have multiple bleeding risk factors that may induce physicians to avoid anticoagulation and because previous studies failed to provide convincing evidence of the effect on mortality. If on the one hand this finding supports the treatment of patients with SVT, in particular by suggesting a possible safety benefit associated with recanalization and prevention of new onset or worsening of portal hypertension, on the other hand we acknowledge that selection bias related to the choice of not treating sicker patients and those with a poor prognosis may have had an impact on our results.
The current work has several limitations that warrant discussion. First, the studies included patients who were heterogenous in their characteristics, underlying risk factors, vein involvement, anticoagulant treatment, and duration of follow-up. This variability may have resulted in the high heterogeneity of effects of anticoagulant therapy and may affect the external validity of the results. The size of the study population and the availability of some clinical and study-related variables enabled us to explore interstudy heterogeneity, which was only partly explained by the analysis, however, leaving the risk for residual confounding. Second, the evaluation of all outcomes on a study-level basis represents an intrinsic design limitation of a study-level meta-analysis and hampered an in-depth analysis of the impact of specific characteristics (eg, site of thrombosis or different anticoagulant treatments) on the outcomes. Similarly, the efficacy and safety of anticoagulant therapy could not be assessed in relation to patient-specific risk factors like solid cancer or myeloproliferative neoplasms. Subgroup and sensitivity analyses suggested that the effects of anticoagulant treatment on radiological and clinical outcomes were consistent across different subgroups of patients, including those with liver cirrhosis. Third, all included studies were at risk of bias (supplemental Table 3; supplemental Figures 1 and 2), which potentially limits the external validity of the results and emphasizes the urgent need for high-level evidence in this field. Fourth, only 1 study randomized patients to anticoagulant therapy vs no treatment.28 All measures of effect were largely derived from cohort studies in which the decision to use a specific agent or withhold anticoagulation was not randomized and could be influenced by patient characteristics and prognosis. Therefore, all comparisons among different types of anticoagulant agents or between anticoagulation and no treatment remain exploratory and should be viewed cautiously. A proportion of patients received concomitant antiplatelet therapy, mostly those with underlying myeloproliferative neoplasms. Poor reporting precluded additional analysis on this subgroup of patients. Finally, there was evidence of significant publication bias for the effects of anticoagulant treatment on progression of SVT, major bleeding, and overall mortality. This finding is consistent with the possibility that small studies with large effect size were not published. However, it is unlikely that the latter were missed by our systematic search that considered several databases without study size restriction.
In summary, anticoagulant therapy for SVT is associated with vein recanalization and low probability of thrombosis progression. The risks of recurrent VTE and major bleeding in patients receiving anticoagulation therapy and the proportion of events in those left untreated strongly suggest the need for additional studies to optimize SVT management.
For original data, please contact Emanuele Valeriani at emanuele.valeriani@outlook.com.
The online version of this article contains a data supplement.
The publication costs of this article were defrayed in part by page charge payment. Therefore, and solely to indicate this fact, this article is hereby marked “advertisement” in accordance with 18 USC section 1734.
Acknowledgments
The authors thank T. Artaza, L. Benjilali, G. Coltro, B. A. Derman, H. C. Kwaan, E. Sant’Antonio, K. K. Søgaard, A. Tosetto, A. M. Vannucchi, and K. T. Werner, who provided additional data needed for the analysis.
Authorship
Contribution: E.V., M.D.N., N.R., and W.A. were responsible for the conception and design of the study; E.V., O.C., M.D.N., and N.R., acquired the data; E.V., M.D.N., and N.R. performed the statistical analyses; and all authors interpretated the data, drafted the manuscript, made critical revisions of the manuscript for important intellectual content, and provided final approval of the manuscript.
Conflict-of-interest disclosure: M.D.N. reports personal fees outside the submitted work from Bayer, Daiichi Sankyo, Pfizer, Leo Pharma, and Aspen. W.A. received a research grant from Bayer to support a clinical study in patients with splanchnic vein thrombosis; received honoraria for serving on advisory boards of Bayer, Boehringer Ingelheim, Daiichi Sankyo, BMS/Pfizer, Sanofi, and Portola; and received grants and personal fees outside the submitted work from Bayer, and personal fees from BMS/Pfizer, Daiichi Sankyo, Sanofi, Aspen, Janssen, and Portola. The remaining authors declare no competing financial interests.
Correspondence: Emanuele Valeriani, Department of Medical, Oral and Biotechnological Sciences, “G. d’Annunzio” University, Via Dei Vestini 31, 66100 Chieti, Italy; e-mail: emanuele.valeriani@outlook.com.
