

In this issue of Blood, 1 report encouraging results from a randomized, multicenter, phase 2 trial (the ROCKstar Study) of treatment with the ROCK2 inhibitor belumosudil in patients with inadequately controlled chronic graft-versus-host disease (cGVHD) after 2 or more lines of prior therapy.
When dire diseases are cured by allogeneic hematopoietic cell transplantation, patients still face many obstacles in their struggle to return to normal. Among them, cGVHD is a leading cause of nonrelapse mortality and morbidity. Between 35% and 70% of patients develop cGVHD with 30% to 50% of them having steroid-refractory or steroid-dependent cGVHD. After starting initial systemic therapy for National Institute of Health (NIH)-defined moderate or severe cGVHD, only 1 of 3 patients will be alive and off immunosuppression 5 years later.2 This significant burden of GVHD in survivors has led to the introduction of a composite end point of cGVHD plus relapse-free survival. Manifestations of cGVHD are heterogenous and affect multiple organs. Among them, keratoconjunctivitis sicca, sclerosis, bronchiolitis obliterans, severe joint/fascia involvement, and esophageal strictures are the most frequently associated with high morbidity3 and impaired quality of life. Hence, the big question in the field is how to control cGVHD without increasing the risk of serious adverse effects from immunosuppressive treatment.
Cutler et al show that selective inhibition of ρηo-associated, coiled-coil–containing protein kinase 2 (ROCK2) with belumosudil (formerly known as KD025) is effective and safe in heavily pretreated patients with persistent cGVHD manifestations after 2 to 5 prior systemic lines of therapy (LOTs). The authors are to be congratulated for this trial in these difficult-to-treat patients with advanced stages of cGVHD. Two-thirds of patients had NIH-defined severe cGVHD. Prior treatment included a median of 3 prior LOTs with 27% having at least 5 LOTs. Many of the patients had received extracorporeal photopheresis, ibrutinib, and/or ruxolitinib. Half of patients had 4 or more organs involved, with a high percentage with skin, joints/fascia, eye, mouth, lung, and/or esophagus involvement. High overall response rates (ORRs) were observed across different organs and prior treatment histories, with partial responses being more frequently recorded in manifestations where fibrosis or permanent organ damage dominated, such as joint/fascia, eyes, skin, or lungs (see figure). Notably, most patients receiving prior ibrutinib or ruxolitinib therapy responded to belumosudil, and adverse events were within the expected spectrum for this patient population, with rather few infectious complications. More data from ongoing surveillance are needed to further our understanding of the adverse event profile of belumosudil.
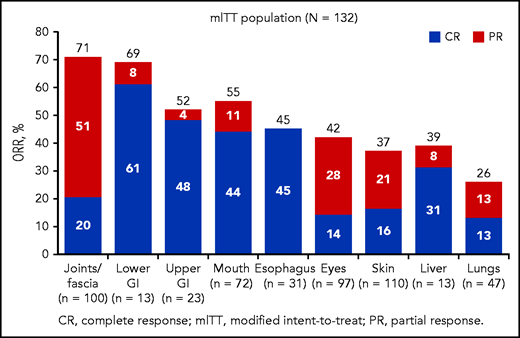
Overall response rate by organ system in patients receiving at least 1 dose of belumosudil. See Figure 3 in the article by Cutler et al that begins on page 2278.
Overall response rate by organ system in patients receiving at least 1 dose of belumosudil. See Figure 3 in the article by Cutler et al that begins on page 2278.
The ROCKstar Study is highly valuable. It demonstrates that selective inhibition of ROCK2 by belumosudil provides a new therapeutic strategy, targeting both immune dysregulation and fibrosis. Use of ROCK2 inhibition for treatment of cGVHD is the result of a deeper understanding of pathogenesis, mainly originating from animal models but also from human data. It is a complex and heterogenous immunological reaction including inflammation and T- and B-cellular and humoral immune dysregulation, among others characterized by a low number of regulatory T (Treg) cells, activation of T follicular helper (Tfh) cells, and promotion of antibody production against host antigens by B cells. Fibrosis is thought to be initiated by several pathways involving antibodies, Tfh cells, and type 17 T helper (Th17) cells (Th17), with stimulation of macrophages, fibroblast proliferation, and accumulation of extracellular matrix.4 Previous work has shown that ROCK2 exerts multiple effects by activating downstream substrates involved in T-cell plasticity and macrophage polarization, restoring the balance between immune cells (ie, the Th17/Tfh/Treg balance, as well as the balance between M1- and M2-type macrophages).5 Hence, these pathways offer several potential targets for selective ROCK2 inhibition in cGVHD.
In multiple murine models, belumosudil ameliorated sclerodermatous cGVHD or bronchiolitis obliterans. This effect was associated with a decreased frequency of Tfh cells and increased frequency of T follicular regulatory cells accompanied by a reduction in phosphorylated signal transducer and activator of transcription 3 (pSTAT3) and concurrent increase in STAT5 phosphorylation.6 The initial data on safety and efficacy were then collected from 54 patients with cGVHD in a phase 2 dose-finding study that has recently been published.7
The ROCKstar Study reports encouraging response rates. No clinically significant difference in efficacy or safety was noted between the 2 compared doses of belumosudil (200 mg twice daily and 200 mg per day), suggesting further exploration of the minimal effective dose in this patient population. cGVHD pathways are diverse, and so are disease manifestations, factors that are also apparent in the ROCKstar Study. Despite a high ORR, some patients discontinued the study drug because of progression of cGVHD or inability to reduce the steroid dose. Hence, it is unlikely that belumosudil will be rockin’ GVHD treatment from the ground, at least not yet. However, with belumosudil, ibrutinib,8 and ruxolitinib,9 3 agents with different mechanisms of action are enlarging our therapeutic armamentarium for difficult to treat cGVHD in the recent years, more will certainly follow. The question will be when to use which therapy at what time. It is likely that we will use these drugs for different profiles and at different times in the course of the disease, after further study in randomized clinical trials. Combining therapies may prevent bypass effects of the dysregulated immune system that could otherwise occur. And, last but not least, these drugs need also to be further explored for early treatment of cGVHD, including first-line treatment instead of steroids,10 or even for cGVHD prevention. Obviously, biomarkers will become another important mainstay to guide decision making.
Removing the mountain called GVHD starts with crushing rocks to stones that will finally be used to pave roads for a better life for transplant survivors. One of these stones is now being called ROCKStar.
Conflict-of-interest disclosure: The author declares no competing financial interests.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal