

Key Points
Anti–SARS-CoV-2 vaccination leads to lower production of antibodies in WM patients.
Treatment with rituximab or BTK inhibitors was an independent prognostic factor for suboptimal antibody response after vaccination.

Abstract
Immunocompromised patients with hematologic malignancies are more susceptible to COVID-19 and at higher risk of severe complications and worse outcomes compared with the general population. In this context, we evaluated the humoral response by determining the titers of neutralizing antibodies (NAbs) against SARS-CoV-2 in patients with Waldenström macroglobulinemia (WM) after vaccination with the BNT162b2 or AZD1222 vaccine. A US Food and Drug Administration–approved enzyme-linked immunosorbent assay–based methodology was implemented to evaluate NAbs on the day of the first vaccine shot, as well as on days 22 and 50 afterward. A total of 106 patients with WM (43% men; median age, 73 years) and 212 healthy controls (46% men; median age, 66 years) who were vaccinated during the same period at the same center were enrolled in the study (which is registered at www.clinicaltrials.gov as #NCT04743388). Our data indicate that vaccination with either 2 doses of the BNT162b2 or 1 dose of the AZD1222 vaccine leads to lower production of NAbs against SARS-CoV-2 in patients with WM compared with controls on days 22 and 50 (P < .001 for all comparisons). Disease-related immune dysregulation and therapy-related immunosuppression are involved in the low humoral response. Importantly, active treatment with either rituximab or Bruton’s tyrosine kinase inhibitors was proven as an independent prognostic factor for suboptimal antibody response after vaccination. In conclusion, patients with WM have low humoral response after COVID-19 vaccination, which underlines the need for timely vaccination ideally during a treatment-free period and for continuous vigilance on infection control measures.
Introduction
The new type of coronavirus SARS-CoV-2, which originated from Wuhan, China, has led to the worldwide pandemic of coronavirus disease–2019 (COVID-19) and has become a global health concern.1,2 COVID-19 is a systemic disease with both short- and long-term manifestations.3,4 Most patients present with mild to moderate symptoms; however, up to 5% to 10% present with a severe and even life-threatening disease course.3 Mitigation measures such as physical distancing and universal mask wearing are particularly important against COVID-19 transmission. However, herd immunity can be attained only with the implementation of effective and safe vaccines against SARS-CoV-2.5,6 The urgency of the COVID-19 pandemic led to accelerated vaccine development within less than a year.7 Several phase 3 placebo-controlled, randomized clinical trials were performed and showed impressive efficacy for different vaccine types; however, the effectiveness and the durability of protection in real world is still under investigation.8 Considering that very few patients with underlying malignancies were enrolled in those studies, several questions remain unanswered regarding the risk-benefit ratio of these new COVID-19 vaccines in patients with cancer.7,9
Immunocompromised patients with hematologic malignancies or solid cancer are more susceptible to COVID-19 and present a higher risk of severe complications and worse outcomes compared with the general population.10,11 Additionally, the subgroup of patients with hematologic malignancies seem to have worse clinical outcomes with higher morbidity and mortality compared with patients with solid organ tumors.12 Among hospitalized patients with COVID-19 and hematologic cancers, the risk of death has been estimated at approximately 39%.12 Furthermore, lower seroconversion rates after COVID-19 have been reported among patients with solid and hematologic cancer compared with convalescent individuals without cancer.13-16
Waldenström macroglobulinemia (WM) is a rare subgroup of indolent B-cell lymphomas. It is defined by the presence of a monoclonal immunoglobulin M (IgM) serum protein and at least 10% monoclonal lymphoplasmacytic cells in the bone marrow. WM accounts for 1% to 2% of all hematologic malignancies.17 Patients with lymphoproliferative disorders including WM are at increased risk of bacterial and viral infections and also at increased risk for severe disease and death from COVID-19 because of their immunocompromised status, older age, and comorbidities.18-23
Herein, we describe the humoral response, as depicted by the development of neutralizing antibodies (NAbs), against SARS-CoV-2 in patients with WM after vaccination with either the mRNA BNT162b2 or the viral vector AZD1222 vaccine.
Patients and methods
Patients and controls
Major inclusion criteria for the study included the following: (1) age above 18 years; (2) presence of asymptomatic or active WM irrespective of the treatment phase; and (3) eligibility for vaccination. Volunteer controls of similar age were also included in this analysis. We included healthy individuals without malignant disease older than 60 years of age vaccinated during the same time period (January-May 2021). The age cutoff was selected taking into consideration the median age of patients with WM23 and the age groups that were prioritized according to the National Vaccination Program. Major exclusion criteria for both patients and controls included the presence of (1) autoimmune disorders or active malignant disease besides WM; (1) HIV or active hepatitis B and C infection; and (3) end-stage renal disease. These disease entities were excluded because of concerns of confounding effect on antibody response after vaccination. Relevant data were extracted from the medical records and included demographics, complete blood count, serum immunoglobulin levels, disease status, and type of treatment.
All participants (patients with WM and controls) have been enrolled in a large prospective study (#NCT04743388) evaluating the kinetics of anti–SARS-CoV-2 antibodies after COVID-19 vaccination in healthy subjects and patients with hematologic malignancies or solid tumors. According to the National Vaccination Program in Greece, the 2 doses of BNT162b2 are administered 3 weeks apart, whereas the 2 doses of AZD1222 are given 3 months apart. The study was approved by the Institutional Ethics Committee of General Hospital Alexandra, Athens, Greece, in accordance with the Declaration of Helsinki and the International Conference on Harmonization for Good Clinical Practice. All patients and controls provided written informed consent prior enrollment in the study.
NAb measurement
After vein puncture, the serum of both patients and controls was collected on day 1 (D1; before the first BNT162b2 or AZD1222 dose), on day 22 (D22; before the second dose of the BNT162b2 or 3 weeks after the first AZD1222 dose), and on day 50 (D50; 3 weeks after the second dose of the BNT162b2 or 6 weeks after the first AZD1222 dose). Serum was separated within 4 hours of blood collection and stored at −80°C until the day of measurement. NAbs against SARS-CoV-2 were measured using US Food and Drug Administration–approved methodology (enzyme-linked immunosorbent assay, cPass SARS-CoV-2 NAbs Detection Kit; GenScript, Piscataway, NJ)24 on the abovementioned time points. An NAb titer of at least 30% is considered as positive, whereas an NAb titer of at least 50% has been associated with clinically relevant viral inhibition.25 Samples of the same patient or control were measured in the same enzyme-linked immunosorbent assay plate.
Statistical analysis
All statistical analyses were performed with STATA (version 17.0, College Station, TX). All variables were tested for normal data distribution. The analyses were performed on an intention-to-treat and on-treatment basis. Normally distributed data were expressed as means ± standard deviation (SD). Non-normally distributed data were presented as the median with the interquartile range (IQR). For categorical variables, the χ2 or Fisher exact test was used to compare the distributions for the 2 randomized groups. Nonpaired Student t tests were used for between-treatment comparisons of continuous variables. Post hoc mixed-model repeated-measures analysis was used to evaluate the neutralizing antibodies over time with cases and controls as main effects and neutralizing antibodies as dependent variables. Mixed models were performed using direct likelihood estimation with fixed effects of groups, time of antibodies, and interaction of groups (cases, controls) by timing of antibody measurement. An unstructured covariance matrix was used to model within-patient error. We also used a multivariable linear regression model adjusted for age, sex, active therapy, presence of asymptomatic WM, type of vaccine, uninvolved immunoglobulin levels, and lymphocyte count to evaluate the effect of these factors on NAb production at D22 and D50. NAbs, age, lymphocyte count, and immunoglobulins were inserted as linear variables, and the remaining were inserted as categorical variables. All significance tests were 2 tailed and conducted at the 5% significance level.
Results
Baseline characteristics of patients and controls
The study population included 106 patients (46 men [43%])/60 women [57%]; median age: 73 years; IQR: 64-81 years) and 212 controls (98 men [46%]/114 women [54%]; median age: 66 years; IQR: 62-82 years; P = .36 for comparisons regarding age and sex, respectively). All participants were vaccinated during the same period (1 January 2021-31 May 2021) and at the same vaccination center (Alexandra General Hospital, Athens, Greece). The patients were vaccinated based on the Greek vaccination program that prioritizes patients with malignancies for COVID-19 immunization. Ninety patients (84.9%) were vaccinated with the BNT162b2 and 16 (15.1%) with the AZD1222 vaccine. The distribution of vaccines among patients with WM was similar to controls: 174 (82.1%) controls were vaccinated with the BNT162b2 and 38 (17.9%) with the AZD1222 vaccine (P = .5).
The characteristics of the patients with WM are depicted in Table 1. At the time of vaccination, 33 (42.3%) of 78 symptomatic patients were receiving therapy, 45 (57.7%) were in remission after prior treatment and did not receive any therapy at the time of vaccination, and 28 of 106 (26.4%) patients had asymptomatic disease without current or prior treatment. Active treatment was defined as WM-specific treatment with either chemotherapy or immunotherapy or targeted therapy and their combinations in the last 30 days. Among the patients with symptomatic WM without active treatment, the median time from last treatment dose was 39 (range, 13-162) months.
Characteristics of patients with WM
| Variables | Number of patients |
|---|---|
| Number of patients (male/female, n) | 106 (46/60) |
| Age in years, median (IQR) | 73 (64-81) |
| Symptomatic WM Asymptomatic WM | n = 78 (73.5%) n = 28 (26.5) |
| Vaccination with BNT162b2 | n = 90 (67 symptomatic and 23 asymptomatic) (84.9%) |
| Vaccination with AZD1222 | n = 16 (11 symptomatic and 5 asymptomatic) (15.1%) |
| Patients on active treatment at the time of vaccination Type of therapy | n = 33/78 (42.3%) Rituximab-ibrutinib: n = 16 BTKi monotherapy (ibrutinib, acalabrutinib, zanubrutinib): n = 16 Rituximab: n = 1 |
| Comorbidities | Pulmonary disease: n = 7 (6.6%) Diabetes mellitus: n = 9 (8.5%) Autoimmune disease: n = 4 (3.8%) Cardiovascular disease: n = 48 (45.3%) |
| Immunoglobulins, median ± SD, mg/dL | IgG: 762.6 ± 627 IgA: 96 ± 83.7 IgM: 1338 ± 1436 |
| Total lymphocyte count, median ± SD, cells/mm3 | 2030 ± 1206 |
| Variables | Number of patients |
|---|---|
| Number of patients (male/female, n) | 106 (46/60) |
| Age in years, median (IQR) | 73 (64-81) |
| Symptomatic WM Asymptomatic WM | n = 78 (73.5%) n = 28 (26.5) |
| Vaccination with BNT162b2 | n = 90 (67 symptomatic and 23 asymptomatic) (84.9%) |
| Vaccination with AZD1222 | n = 16 (11 symptomatic and 5 asymptomatic) (15.1%) |
| Patients on active treatment at the time of vaccination Type of therapy | n = 33/78 (42.3%) Rituximab-ibrutinib: n = 16 BTKi monotherapy (ibrutinib, acalabrutinib, zanubrutinib): n = 16 Rituximab: n = 1 |
| Comorbidities | Pulmonary disease: n = 7 (6.6%) Diabetes mellitus: n = 9 (8.5%) Autoimmune disease: n = 4 (3.8%) Cardiovascular disease: n = 48 (45.3%) |
| Immunoglobulins, median ± SD, mg/dL | IgG: 762.6 ± 627 IgA: 96 ± 83.7 IgM: 1338 ± 1436 |
| Total lymphocyte count, median ± SD, cells/mm3 | 2030 ± 1206 |
Humoral response in WM patients and controls
On D1, 10 (9.4%) patients and 19 (10.7%) controls had NAb titers of ≥30% (positivity cutoff); there was no difference regarding the NAb titers between patients and controls on D1 (P = .74). None of them had a prior history of known COVID-19. After the first dose of the vaccine, on D22, WM patients had lower NAb titers compared with controls: the median NAb inhibition titer was 20.5% (IQR: 10%-37%) for WM patients vs 39.8% (IQR: 21.9%-53.4%) for controls (P < .001; Figure 1). More specifically, only 34% (36 of 106) of the patients vs 65% (138 of 212) of controls developed NAb titers ≥30% on D22 (P < .001). The respective number of patients and controls who developed NAb titers ≥50% was 19.8% (21 of 106) and 32.6% (69 of 212), respectively (P = .001; Figure 1).
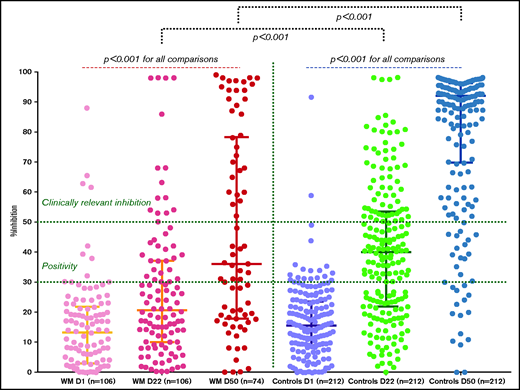
Kinetics of NAbs in patients with WM compared with controls after vaccination with 2 doses of the BNT162b2 or 1 dose of the AZD1222 vaccine. On day 22, patients had lower NAb inhibition titers compared with controls (see text). Only 21 of 106 (19.8%) patients had NAb titers of equal or more than 50%. Similarly, patients had lower NAb inhibition titers compared with controls on day 50 (see text). Only 31 of 74 (42%) patients had NAb titers of equal or more than 50%.
Kinetics of NAbs in patients with WM compared with controls after vaccination with 2 doses of the BNT162b2 or 1 dose of the AZD1222 vaccine. On day 22, patients had lower NAb inhibition titers compared with controls (see text). Only 21 of 106 (19.8%) patients had NAb titers of equal or more than 50%. Similarly, patients had lower NAb inhibition titers compared with controls on day 50 (see text). Only 31 of 74 (42%) patients had NAb titers of equal or more than 50%.
After the second dose of the vaccine, on D50, WM patients had lower NAb titers compared with controls. The median NAb inhibition titer was 36% (IQR: 18%-78%) for WM patients vs 92% (IQR: 70%-96%) for controls (P < .001; Figure 1). NAb data on D50 were available for 74 WM cases. More specifically, only 60.8% (45 of 74) of the patients vs 92.5% (196 of 212) of the controls developed NAb titers ≥30% on D50 (P < .001). The respective number of patients and controls who developed NAb titers ≥50% was 42% (31 of 74) and 85.4% (181 of 212), respectively (P < .001; Figure 1). Among these high-responder patients (n = 31), 19 had symptomatic WM and 12 had asymptomatic WM. In the group of 19 patients with symptomatic WM, 17 were in remission (complete or partial) without receiving any therapy (all 17 patients were off treatment for more than 12 months) and 2 were receiving active treatment with rituximab-ibrutinib and ibrutinib alone, respectively. All patients who achieved clinically relevant humoral response (NAb titers ≥50%) had the uninvolved immunoglobulins within normal limits. Among the patients with low response rates (<30%) at D50 (n = 29), 25 were symptomatic and 4 were asymptomatic. Among the 25 patients with symptomatic WM, 12 were on active treatment at the time of vaccination; 6 patients were receiving ibrutinib with rituximab, and 6 were receiving monotherapy with a Bruton’s tyrosine kinase inhibitor (BTKi; 4 with ibrutinib, 1 with acalabrutinib, and 1 with zanubrutinib). The other patients were previously treated but not on active treatment.
Predictive factors for NAb production
Among patients with WM, there was a trend toward higher NAb production at day 22 with the BNT162b2 mRNA vaccine compared with the AZD1222 vaccine (median, 28.2% vs 17.3%, respectively; P = .076), whereas the difference became more prominent and statistically significant at D50 (median, 52% vs 21.8%, respectively; P = .02). Similar to patients, NAb production was superior in controls vaccinated with BNT162b2 compared with those vaccinated with AZD1222 (median NAbs at day 50: 87.4% vs 47.5%, respectively; P < .001). Furthermore, although there were no significant differences at baseline regarding NAb levels between patients and healthy controls, patients with WM showed an inferior NAb response in all subsequent time points (D22 and D50) compared with controls (P < .05 for all comparisons), regardless the type of vaccine received (ie, BNT162b2 [Table 2] or AZD1222 [Table 3]).
Neutralizing antibodies among cases and controls vaccinated with the BNT162b2 CoV-19 vaccine
| Variables | WM(n = 90) | Controls(n = 174) | P |
|---|---|---|---|
| NAb, day 1 (%) | 15 ± 1.7 | 16.6 ± 1 | .37 |
| NAb, day 22 (%) | 28.2 ± 2.5 | 41.3 ± 1.8 | <.001 |
| NAb, day 50 (%) | 52 ± 4.3 | 87.4 ± 1.3 | <.001 |
| Percentage over 30% NAb, day 1 | 10% | 11.8% | .66 |
| Percentage over 30% NAb, day 22 | 37.8% | 67.5% | <.001 |
| Percentage over 50% NAb, day 22 | 16.7% | 33.1% | .005 |
| Percentage over 30% NAb, day 50 | 68.9% | 97.7% | <.001 |
| Percentage over 50% NAb, day 50 | 50.8% | 94.3% | <.001 |
| Variables | WM(n = 90) | Controls(n = 174) | P |
|---|---|---|---|
| NAb, day 1 (%) | 15 ± 1.7 | 16.6 ± 1 | .37 |
| NAb, day 22 (%) | 28.2 ± 2.5 | 41.3 ± 1.8 | <.001 |
| NAb, day 50 (%) | 52 ± 4.3 | 87.4 ± 1.3 | <.001 |
| Percentage over 30% NAb, day 1 | 10% | 11.8% | .66 |
| Percentage over 30% NAb, day 22 | 37.8% | 67.5% | <.001 |
| Percentage over 50% NAb, day 22 | 16.7% | 33.1% | .005 |
| Percentage over 30% NAb, day 50 | 68.9% | 97.7% | <.001 |
| Percentage over 50% NAb, day 50 | 50.8% | 94.3% | <.001 |
Values are expressed as median ± IQR or as percentages (%). Bold values denote statistical significance.
Neutralizing antibodies among cases and controls vaccinated with the ChAdOx1 CoV-19 vaccine
| Variables | WM(n = 16) | Controls(n = 38) | P |
|---|---|---|---|
| NAb, day 1 (%) | 16 ± 10 | 16.3 ± 9.7 | .9 |
| NAb, day 22 (%) | 17.3 ± 2.4 | 34.6 ± 3.7 | .005 |
| NAb, day 50 (%) | 21.8 ± 2.6 | 45.5 ± 3.8 | <.001 |
| Percentage over 30% NAb, day 1 | 6.3% | 3.9% | .7 |
| Percentage over 30% NAb, day 22 | 12.5% | 52.6% | .006 |
| Percentage over 50% NAb, day 22 | 0% | 29% | .016 |
| Percentage over 30% NAb, day 50 | 23% | 68.4% | .004 |
| Percentage over 50% NAb, day 50 | 0% | 44.7% | .003 |
| Variables | WM(n = 16) | Controls(n = 38) | P |
|---|---|---|---|
| NAb, day 1 (%) | 16 ± 10 | 16.3 ± 9.7 | .9 |
| NAb, day 22 (%) | 17.3 ± 2.4 | 34.6 ± 3.7 | .005 |
| NAb, day 50 (%) | 21.8 ± 2.6 | 45.5 ± 3.8 | <.001 |
| Percentage over 30% NAb, day 1 | 6.3% | 3.9% | .7 |
| Percentage over 30% NAb, day 22 | 12.5% | 52.6% | .006 |
| Percentage over 50% NAb, day 22 | 0% | 29% | .016 |
| Percentage over 30% NAb, day 50 | 23% | 68.4% | .004 |
| Percentage over 50% NAb, day 50 | 0% | 44.7% | .003 |
Values are expressed as median ± IQR or as percentages (%). Bold values denote statistical significance.
In the group of patients with WM, there was no significant difference between the asymptomatic and symptomatic patient subgroups regarding the titers of NAbs both at D22 (P = .46) and D50 (P = .3). A numerical trend in favor of the asymptomatic subgroup was found at D50 (median NAbs, 52.9% vs 44.3%, respectively).
Among the patients with symptomatic disease, the subgroup treated with a BTKi had lower median NAbs titers compared with other symptomatic patients at D22 (13.6% vs 32.6%, respectively; P < .001) and D50 (median, 27.8% vs 50.8%, respectively; P = .03). The subgroup of symptomatic patients treated with rituximab-based combinations (rituximab-cyclophosphamide-dexamethasone-bortezomib, rituximab-bendamustine, rituximab-ixazomib-dexamethasone, rituximab-ibrutinib with or without bortezomib) in the last 12 months exhibited impaired humoral response at D22 (median NAbs, 11.9% vs 29.3% among other symptomatic patients, respectively; P = .007) and D50 (median NAbs, 22.3% vs 48.8%, respectively; P = .04).
Our analysis did not identify an interaction between age and NAb titers at D22 (P = .09) and D50 (P = .07). No correlations were identified between sex, body mass index, lymphocyte count at baseline, and NAb production in patients with WM. Among patients with WM, a multivariable linear regression model adjusted for age, sex, active therapy, presence of asymptomatic WM, type of vaccine, uninvolved immunoglobulin levels, and lymphocyte count showed that receipt of active therapy (β coefficient, −0.52; P < .001) was independently associated with reduced levels of NAbs at D22. Also, active therapy was associated with reduced NAb response at D50 after vaccination (β coefficient, −0.4; P = .001).
Adverse events
Among patients with WM, 33 of 90 (37%) and 34 of 90 (38%) reported mild reactions after the first and second dose of the BNT162b2 vaccine, respectively. Thirty-one percent of the patients (5 of 16) vaccinated with the first dose of AZD1222 presented with local reactions as well. These reactions included mainly pain at the site of the injection, erythema, and/or swelling. The rate of this adverse event between the first and second dose of BNT162b2 was not statistically significant (P = .7). Thirteen percent (12 of 90) and 24% (22 of 90) of the patients vaccinated with the BNT162b2 vaccine reported systemic adverse reactions after the first and second vaccine shot, respectively, but all were categorized as mild. The systemic adverse events included fatigue, fever, lymphadenopathy, muscle pain, arthargias, and headache. The emergence of the adverse events related to vaccination was independent of the active treatment or disease status.
Discussion
Our data indicate that vaccination with either the BNT162b2 mRNA vaccine or the AZD1222 viral vector vaccine leads to lower production of NAbs against SARS-CoV-2 in patients with symptomatic and asymptomatic WM compared with controls of similar age and sex without malignant disease. Our findings were independent of the vaccine type. Interestingly, the sex distribution of the WM cases included more women than men, which is not typical for WM.23 However, it could be attributed to a higher rate of anti–SARS-CoV-2 vaccine uptake among women compared with men because of sex-specific and societal reasons.26 To our knowledge, this is the first report to demonstrate the antibody-mediated response in patients with WM after 2 doses of vaccination with the BNT162b2 vaccine. Furthermore, it is the first study demonstrating the effects of AZD1222 vaccine in patients with low-grade lymphoproliferative neoplasms.
Although vaccination against SARS-CoV-2 is considered as the most important preventive strategy against COVID-19, its efficacy in patients with hematologic malignancies is largely unknown.9 The BNT162b2 mRNA and AZD1222 viral vector vaccines against SARS-CoV-2 have shown significant efficacy in healthy adults.27,28 BNT162b2 is a lipid nanoparticle-formulated, nucleoside-modified RNA vaccine that encodes a prefusion stabilized, membrane-anchored SARS-CoV-2 full-length spike protein. The ChAdOx1 nCoV-19 vaccine (AZD1222) was developed at Oxford University and consists of a replication-deficient chimpanzee adenoviral vector ChAdOx1, containing the SARS-CoV-2 structural surface glycoprotein antigen (spike protein; nCoV-19) gene. The first BNT162b2 dose confers some protection among nursing facility members,29,30 health care workers, and octogenarians.31 However, among 167 patients with chronic lymphocytic leukemia (CLL), only 39.5% had a positive antibody-mediated response to the BNT162b2 vaccine.32 Low antibody responses have been also reported among 48 elderly patients with myeloma who received the first dose of BNT162b2 vaccine.33 A suboptimal immune response to vaccines in those patients may be attributed to defects in immune effector cells, associated with both the underlying B-cell disorder and the therapeutic approaches.32-34
The underlying causes for low humoral response to vaccination in patients with WM are multifactorial, and it seems that both disease-related immune dysregulation and therapy-related immunosuppression are involved. In our study, active treatment (with rituximab, BTKi, or combinations) was the most important prognostic factor at the multivariate analysis and was correlated with lower response rates.
Therapeutic regimens that deplete B cells may impair immune response to vaccines. Patients treated with ibrutinib and/or anti-CD20 antibodies were unlikely to respond to a single dose of vaccine, and this was confirmed by our results. BTKis, including ibrutinib, acalabrutinib, and zanubrutinib, block B-cell receptor signaling in both malignant and normal B cells, and therefore, it impairs the humoral response to vaccination.35-38 Previous studies have described antibody-mediated response rates of 7% to 26% to the influenza vaccine in patients with CLL treated with BTKis.35,36 It has been also demonstrated that BTKis are associated with a decreased immune response to the anti–hepatitis B vaccine, HepB-CpG19.39 Furthermore, we showed that patients with WM treated with an anti-CD20 antibody within the last 12 months before vaccination failed to produce anti–SARS-CoV-2 antibodies, whereas better responses were observed in patients who completed anti-CD20 therapy at least 12 months before vaccination. The recent exposure to B cell–depleting agents, including anti-CD20 antibodies, reduces response to the influenza vaccine, pneumococcal polysaccharide vaccine, and other vaccines.40,41 Interestingly, hypoglobulinemia might be associated with inferior antibody response among patients with CLL and COVID-19.16 Furthermore, it seems that patients who completed their treatment and remained in response at the time of vaccination were more likely to produce NAbs, and this is probably related to a reconstitution of humoral immunity. In this context, the delay of treatment initiation may be considered when possible until the vaccination is completed. Although targeted therapies seem to negatively affect NAb production, higher patient numbers are required to evaluate the exact effect of each regimen on the immune responses after anti–SARS-CoV-2 vaccination.
Taking into consideration the humoral response after the first and second vaccine shot, it is clearly suggested that a second timely vaccine dose is necessary, especially for patients with hematologic malignancies that deregulate the immune homeostasis. In accordance to a previous study on healthy individuals,42 our results may advocate for a shortening of the time interval between the 2 doses of the AZD1222 to less than 3 months, especially for patients with WM. However, further data in a larger sample size are needed to conduct subgroup analysis and evaluate the peak antibody response from the AZD1222 vaccine compared with the BNT162b2 vaccine.
It is well known that patients with cancer have increased COVID-19–related mortality; however, there is significant heterogeneity among different cancer subgroups.43 Currently, it has been demonstrated that vaccines result in lower risk for severe disease; however, the studies performed were not designed to detect a signal for mortality protection from fatal COVID-19. The available data regarding vulnerable subgroups, such as patients with cancer, are lacking. One of the strengths of our study is the evaluation of NAbs, which have been shown to have an important predictive value of immune protection from symptomatic COVID-19.44 Therefore, NAb levels can be considered valuable surrogates of vaccine efficacy.
Our results suggest that patients with WM have suboptimal production of anti–SARS-CoV-2 NAbs, in analogy to the response to influenza vaccines. Existing data on patients with plasma cell dyscrasias are rather limited, and they are based on small and retrospective studies that suggest poor seroprotection rates of less than 20% after standard influenza vaccination.45 A prospective single-arm study has demonstrated that, in contrary to these historically poor results with standard influenza vaccination, a novel high-dose booster vaccination strategy might lead to high rates of seroprotection.46 Another study has shown decreased antipneumococcal immunity in patients with both multiple myeloma (MM) and WM.47 In addition, these results are in accordance with the low response rates of 20% to 40% to pneumococcal conjugated vaccine (PCV13), pneumococcal polysaccharide vaccine (PPSV23), and HepB-CpG vaccine,38,48-50 as well as of the reduced efficacy of influenza A and B vaccination reported in patients with other lymphoproliferative disorders such as CLL.50
Therefore, the protection of patients with hematologic cancer against severe SARS-CoV-2 infection and reinfection by SARS-CoV-2 variants is still unknown. Although humoral immunity seems to be deregulated, mucosal surface antibodies, such as IgA, and protective T-cell responses, might be similarly or even more important in the protection after natural SARS-CoV-2 infection or vaccination.51,52 However, no such data for patients with cancer are currently available. Memory B-cell and T-cell responses might be significantly compromised in patients with cancer, especially those with hematologic malignancies.53 Further studies on the kinetics of immune subpopulations after COVID-19 vaccination will elucidate the underlying immune landscape and determine the potential need for additional booster doses in patients with B-cell malignancies.
In summary, the antibody-mediated response to SARS-CoV-2 vaccines in patients with WM is considerably affected by both the underlying disease and active treatment. Although the response rates were not optimal, vaccination is still considered essential, and if possible, should be performed before treatment initiation. Larger studies with longer follow-up are needed to understand the rate of actual COVID-19 infections in vaccinated patients with WM. Furthermore, based on our results, it seems reasonable to administer COVID-19 vaccination before cytotoxic chemotherapy, lymphodepleting agents such as monoclonal antibodies, or long-term corticosteroids. In the absence of contraindications, a careful counseling of patients with WM to proceed with vaccination seems appropriate. It might be of interest to evaluate differences in dosing, dosing intervals, and number of boosting doses in these patients. For these patients, prolonged self-protection measures, such as mask wearing and social distancing, are necessary. Finally, the effect of the long-term safety of these vaccines seems reassuring; however, close monitoring is required especially in patients with WM, considering the increased risk for concurrent or synergistic adverse events.
Acknowledgments
The authors thank Ioanna Charitaki, Tina Bagratuni, Christine Ivy Liacos, Nikoletta-Aikaterini Kokkali, Nefeli Mavrianou-Koutsoukou, Dimitrios Patseas, and Stamatia Skourti for administrative, technical, or material support; Sentiljana Gumeni and Eleni-Dimitra Papanagnou for acquisition, analysis, or interpretation of data; and all of the study participants for donating their time and samples. This study was partially funded by SYN-ENOSIS (Greece), AEGEAS (Greece), IEMBITHEK (Greece), Nikos, and Theano Vafeias.
Authorship
Contribution: M.G., E.T., and M.A.D. designed research, performed research, analyzed data, and wrote the paper; A.B., I.P.T., and I.N.-S. contributed vital new reagents or analytical tools, performed research, analyzed data, reviewed all paper drafts, and gave approval to final version; and E.K., S.G., D.F., P.M., E.E.-P., F.T., N.K., and M.M. performed research, analyzed data, reviewed all paper drafts, and gave approval to final version.
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Correspondence: Maria Gavriatopoulou, Department of Clinical Therapeutics, National and Kapodistrian University of Athens, School of Medicine, Alexandra General Hospital, 80 Vas Sofias Ave, 11528 Athens, Greece; e-mail: mgavria@med.uoa.gr.

