
Linus Pauling once stated, “Optimum nutrition is the medicine of tomorrow.” This two-time Nobel laureate first discovered the molecular basis of sickle cell disease (SCD). He also believed that you could trace every sickness, disease, and ailment to a mineral deficiency. While this might not have been borne out over time, certainly modern medicine recognizes the importance of nutrition — both under- and overnutrition — as an important mediator of health and wellness. Nutrition has been touted as a key predictor of the course of various chronic conditions such as diabetes and cardiopulmonary diseases,1 and there have been several reports of global energy and nutrient deficits in SCD.2,3 The amplified catabolism associated with increased red cell turnover of SCD leads to multiple macro- and micronutrient deficiencies, predominantly reported in children. For example, in 2016, Dr. David J. Martyres and colleagues evaluated 91 Canadian children with SCD and noted that 42 percent and 27 percent had multiple- or single-nutrient deficiencies/insufficiency, respectively. The common micronutrient deficits seen in SCD include vitamin D, zinc, folate, and B6 deficiencies — deficiencies linked to an increased number of pain episodes. Zinc deficiency in children with SCD has been associated with growth retardation, cell-mediated immune dysfunction, and cognitive impairment.4 Suboptimal vitamin D status has also been widely reported in both children and adults with SCD across the globe, ranging in prevalence from 33 percent to 100 percent.5,6 Selenium deficits in adults with SCD have been associated with increased hemolysis.7 While these individual reports suggest a role for nutrition in SCD outcomes, the global impact of nutrition status on the severity of SCD and health-related quality of life among adults has not been comprehensively studied.
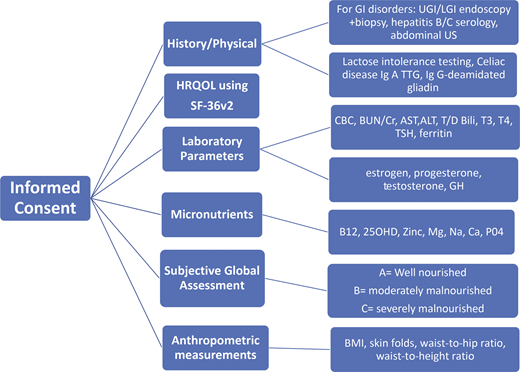
In a longitudinal case-control study by Dr. Sanaa Kamal and colleagues, investigators sought to determine the nutritional determinants of SCD severity in adults, building on work that has been done in children. They followed a cohort of 62 male and female adults with homozygous SS aged 18 years or older for eight years (November 2012-January 2020) along with 50 age-, sex-, and province-matched healthy control participants. Following informed consent, enrolled participants provided a detailed medical history and 48-hour dietary recall, underwent a detailed physical examination, and had laboratory parameters assessed (Figure). Subjective global assessment (SGA) of nutrition was performed in all participants who were then grouped into either SGA rating A (normally nourished), SGA rating B (moderately undernourished), or SGA rating C (severely undernourished). SCD severity was determined using the Sickle Cell Disease Severity Calculator (bios.ugr.es/dss-calculator/index.php) published in 2007 by the Steinberg group. Participants were observed for a median of 93 months (95% CI, 92-94 months).
The main study endpoint was a composite score of admission to the hospital for SCD-related events or death from all causes during the follow-up period. At baseline, only 20 participants (32%) with SCD had no identified macro- or micronutrient deficit (or an SGA rating A), while 42 participants (67.8%) with identified nutrient deficiencies had SGA rating B (n=38, 61.3%) or met criteria for SGA rating C (n=3, 6.5%). Gastrointestinal symptoms (e.g., anorexia, weight loss, nausea, dyspepsia, and abdominal colic) were significantly higher among the undernourished participants. SCD participants with macro- or micro-undernutrition had significantly lower body mass index (BMI), serum 25(OH)D, and zinc levels, with significantly higher serum aspartate transaminase/alanine transaminase and total bilirubin levels compared to participants without macro- or micro-undernutrition. They also developed more vaso-occlusive pain crises, pneumonias, renal complications, and recurrent infections during the follow-up period. Having evidence of undernutrition was associated with a significantly higher incidence rate of SCD-related hospitalizations and higher incidence of death, with a relative risk of 14.42 (95% CI, 0.846-46.2664; p=0.05). There were no deaths in the well-nourished group. Importantly the undernourished group had a higher SCD severity score during follow-up (0.52 ± 0.073 vs. 0.29 ± 0.081 in the well-nourished group; p<0.0001).
Daily energy intake, BMI, and zinc levels inversely correlated to SCD severity score. Results from this study suggest that nutritional status was responsible for 88 percent of the severe SCD outcomes. Using multivariate logistic regression of attributable risk, independent risk factors for more severe SCD and worse outcomes were identified to include being male, energy intake less than 1,600 calories, SGA score B or C, BMI less than 18, hemoglobin less than 6 g/dL, vitamin D levels less than 16 ng/mL, and zinc levels less than 60 ng/dL. As expected, health-related quality of life was also significantly lower in nearly all domains among undernourished participants with SCD compared to well-nourished participants.
While these results are discouraging, all hope is not lost. During the follow-up period, individuals identified as having SGA class B and C malnutrition were evaluated by a nutritionist, with correction of the energy deficit and supplementation with vitamin D and zinc, which led to improvement in signs and symptoms. Furthermore, participants who were started on hydroxyurea upon study entry also demonstrated improvements in clinical outcomes and nutritional status. This implies that what a person eats can and will make a difference in mitigating the macro- and micronutrient deficiencies that are common comorbidities of SCD, owing to its pathophysiology.
The SCD severity calculator, while useful for quantifying an individual’s risk for near-term death thus for guiding provider decisions to intensify therapeutic options, has its limitations. It was only validated in two geographically similar populations (National Institutes of Health and Boston University, both in the northeastern United States). Validation in additional disparate populations is needed to determine its broader applicability. Similarly, this study enrolled only younger (median age, 24.21 ± 3.926 years; 95% CI, 23.21 to 25.21) individuals from two provinces, both located in Saudi Arabia. This limits its generalizability to countries such as the United States, where the median age of a person with SCD is into the fourth decade, or in sub-Saharan Africa where the median age is younger (16-19 years).8
In Brief
This prospective, comprehensive, nutritional assessment study sought to identify the influence of nutrition on the course and severity of SCD in adults. It confirms that continuation of nutritional deficits that begin in childhood persists into adulthood and confers worse prognoses and poor quality of life. This study affords a scientific rationale for prospective nutritional screening and risk mitigation by correcting any identified macro- and micronutrient deficits, in addition to optimizing disease management with treatments such as hydroxyurea. The causes of malnutrition in this cohort are probably not solely related to food deprivation or poverty, but perhaps reduced intake or uptake of macro- and micronutrients resulting from increased metabolic demand, chronic gastrointestinal disease, and sociodemographic preferences and lifestyle factors. Undernutrition is also associated with increased hospitalizations and may lead to a cycle of worse undernutrition.
So how can we incorporate the valuable lessons from this robust research into everyday practice? Providers should consider a thorough nutritional assessment for all adults living with SCD to proactively identify sources of undernutrition and implement interventions to correct them. It is also important to educate individuals living with SCD on the vital importance of maintaining a balanced nutritional status of both micro- and macronutrition via diet and adequate supplementation as needed, because what they eat or don’t eat truly determines who they are going to become.
Competing Interests
Dr. Osunkwo indicated no relevant conflicts of interest.
